An Introduction to Applied Cognitive Psychology - David Groome, Anthony Esgate, Michael W. Eysenck (2016)
Chapter 12. Emotion and cognition
Jenny Yiend
12.1 AN INTRODUCTION TO THINKING AND FEELING
For a long time psychologists have known that how we think can influence how we feel. Different interpretations, or ‘cognitive appraisals’, of situations or events can change our emotional response to those events. One psychologist, Richard Lazarus, demonstrated this in a now classic experiment (Lazarus, 1982; Lazarus and Opton, 1966). He showed participants anxiety-provoking films (for example, a Stone Age circumcision ritual and a gruesome industrial accident) and manipulated how they appraised what was going on by playing different soundtracks designed to encourage participants to think in a particular way about the films. For example, a ‘denial’ soundtrack included statements indicating that one was a safety film, that the people in the films were only actors and that the ritual in the film was not actually painful. Results showed that physiological measures of emotion, such as galvanic skin response (how much you are sweating) and heart rate, were reduced during ‘denial’ when compared with when passively watching the same films. This suggests that how we think can indeed influence how we feel, or to put it another way, cognitive appraisal can convincingly alter emotional response.
One obvious application of this is that we may be able to use our thoughts to control our emotions. Psychologists have investigated this too. One study asked participants to look at emotional pictures selected on the basis of normative data to be negative, for example pictures of snarling dogs, snakes and other frightening animals (Yiend et al., 2008). The researchers wanted to test whether directing attention to different parts of each picture could be used to control participants’ emotional response to the pictures. In one condition consecutive pictures were rated according to ‘how frightening’ they were (‘emotional encoding’, which requires processing the frightening aspects of the picture), and in the other condition pictures were rated according to ‘how planned or arranged by the photographer’ they were (‘planned encoding’, which requires processing the neutral aspects of the picture and ignoring the frightening content). Results (shown in Figure 12.1) revealed that healthy volunteers could indeed control their attention by directing it to different aspects of each picture and that this resulted in a greater emotional response during emotional encoding than during planned encoding. This change in emotional response was reflected both in measures of physiology (the body’s biological expression of emotion) and in neural activity in the amygdala, a region of the brain known to be involved in emotion (Mathews et al., 2004).
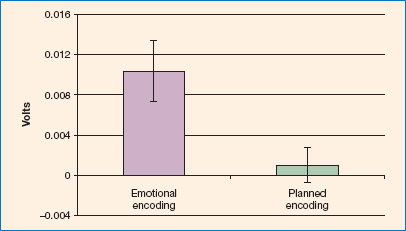
Figure 12.1 Emotional response (eyeblink startle) is greater when participants encode the emotional aspects of a frightening picture (emotional encoding) than when they encode the non-emotional aspects of the same picture (planned encoding).
Source: produced from Yiend et al. (2008). Copyright © 2008 American Psychological Association. Reproduced with permission.
In this short introduction we have seen how different ways of thinking can influence the amount of emotion we experience and how adjusting our thinking is one way to control our emotions. However, emotions and emotional information can also influence, or bias, our ongoing cognitive processes. This is the topic to which we devote the rest of this chapter, both because it is of great current interest to psychologists and because it has a direct application for understanding and treating psychological disorders.
In this chapter we will learn about how and when thoughts affect mood. We will learn how these effects are related to psychological disorders, such as depression and anxiety. We will learn how psychological treatments, such as cognitive behaviour therapy (CBT), work by changing cognitive processes, and in doing so improve psychological disorders, and we will learn about new laboratory-derived techniques, called ‘cognitive bias modification’, that are being developed as new treatments for psychological disorders.
12.2 HOW EMOTIONS AFFECT COGNITION
For a psychologist, the term ‘emotion’ can refer to a variety of different concepts, and from now on in this chapter it will be important to be clear about which one we mean. State emotion, emotional traits and emotional informationare three different meanings of the term ‘emotion’ and all have different effects on cognitive processing. The cognitive effects of these aspects of emotion are frequently called ‘cognitive biases’ because the emotion (whether state, trait or emotional information) can systematically skew cognitive operations such as attention, memory or interpretation. Cognitive biases have been defined as ‘the tendency for the information-processing system to consistently favour stimulus material of a specific content’ (Savulich et al., 2012).
EMOTION STATES
State emotion refers to how you feel right now and this can, of course, change from minute to minute, day to day. State emotion is a very transient and variable entity. It is a construct that allows us to acknowledge the fact that momentary feelings may be quite different from the way an individual normally feels. In some contexts, the term ‘mood’ is used interchangeably with ‘state’, but more commonly experts consider emotional states to be more intense and shorter in duration than moods. Although state emotions are usually measured by self-report (asking participants to introspect and describe how they feel ‘right now’, usually by answering a series of questions using a rating scale or yes/no answers), they can also be measured by how someone behaves (e.g. moving around a lot when agitated or anxious) and by their physiological responses (as mentioned above, things such as heart rate and galvanic skin response).
One popular view assumes that underlying the richness of emotion experience are a small number of discrete emotional states, or ‘basic emotions’ (Ekman, 1992). There is a broad consensus among psychologists that five emotions capture the most fundamental states and are common across all cultures. These are anger, fear, sadness, disgust and happiness. According to some, different combinations of these produce all the other emotions. For example, a mixture of happiness and fear might produce excitement. Facial expressions (see Figure 12.2) are one behavioural way in which we communicate our transient emotional states. Facial expressions are also used by psychologists to study basic emotions, and these expressions are thought to be universally recognised. This approach to describing different emotions is a categorical one; specific discrete categories are listed and named, with little emphasis on varying intensities of emotion or how emotions relate to each other. A different approach is to describe emotions by identifying a few key underlying dimensions such as arousal (a continuous ‘calm’ to ‘excited’ scale) and valence (a continuous ‘positive’ to ‘negative’ scale). Every emotion has a value on both dimensions and can be represented on a two-dimensional emotional map, which can be worked out by asking people to rate how ‘aroused’ and how ‘positive or negative’ they feel about a wide range of emotional material. For example, a picture of a snarling dog would be rated by most people as fairly arousing and quite negative, whereas a picture of a smiling couple would most likely be rated less arousing and reasonably positive. A bit like the coordinates on a geographical map can pinpoint one specific place, the space between one location and another, and the map itself can capture the whole area, so the emotional dimensional map can capture specific emotions, ‘distances’ between emotions and more nuanced variations in emotional intensity. Some researchers consider categorical and dimensional approaches to describing emotion to be complementary to each other, rather than alternatives.

Figure 12.2 Emotion expressions.
Source: copyright g-stockstudio/Shutterstock.com.
As we will see, emotion states can influence cognitive processing quite substantially, although the effects wane as the emotional state dissipates.
EMOTION TRAITS
In contrast to states, emotion traits are stable personality characteristics reflecting ‘what kind of person’ you are and describe how one person may differ from others. For example, some individuals may be prone to angry outbursts, or have a tendency to worry about things, or be optimistic, always looking on the bright side. As with emotion states, they are usually measured using self-report questionnaires. Psychologists have directed much effort into trying to define such personality characteristics, but continue to disagree about how many, and which, are sufficient to describe a person completely. One well-supported view (Eysenck, 1991) proposes a three-factor model of personality comprising the traits of extraversion, psychoticism and neuroticism. Others argue in favour of the ‘Big Five’ personality traits of extraversion, agreeableness, conscientiousness, emotional stability and openness.
A trait tends to make a person more prone to experiencing the associated mood state. For example, a high trait anxious (a trait loosely equivalent to neuroticism) individual will tend to feel more anxious for more of the time than a low trait anxious person. Personality traits can also influence different aspects of cognitive processing, and as you might expect, these effects are enduring and can have important consequences for the individual’s health and well-being.
EMOTIONAL MATERIAL
Another way in which emotion can interact with cognition is when the information that is the subject of cognitive processing is itself emotional. For example, we might observe someone frowning at us, or see an unpleasant image in the newspaper or on television. Psychologists frequently use stimuli like these, which are ‘emotional’, such as positive or negative words or pictures, as a way of studying how we process emotional material. For example, in a typical experiment one might present participants with lists of negative emotional words (e.g. cancer, attack, evil) mixed with neutral words (e.g. number, unusual, round) and ask for later recall in a surprise memory test.
In the psychology of cognition and emotion we are interested not just in how people process emotional material, but also in how this processing is affected by the emotional states and traits described above. For example, does the processing of sad words change when someone is actually feeling sad at the time? Similarly, we might want to know whether people who are vulnerable to anxiety (i.e. high on trait anxiety) process threatening words any differently from those who are not. These more complex questions are what cognition and emotion psychologists are mostly concerned with.
12.3 MEMORY AND EMOTION
Cognitive biases in memory occur when an individual in a current emotional state (for example, happy or sad) recalls emotional information (for example, sad or happy memories). One of the most studied phenomena is mood congruent memory.
MOOD CONGRUENT MEMORY
Mood congruent memory (MCM) refers to what happens to memory processes when the content of material being encoded matches the mood state of the participant doing that encoding. For example, if you are feeling sad and then happen to watch a sad film, your mood is congruent with the film and MCM describes how your sad mood at the time of watching influences your later memory for the film. Bower and colleagues conducted some now classic experiments that sparked a great deal of interest in this phenomenon. In a typical example, participants are put in either a happy or sad mood by hypnosis and then read both a happy and a sad story. Participants are then given a surprise recall test to see how much of each story they can recall. Typical results are shown in Figure 12.3.
As you can see, more was recalled from the story that matched the mood of the participant as they were reading; for example, sad participants recalled more things about the sad story than about the happy one. The phenomenon of MCM has proved very robust.
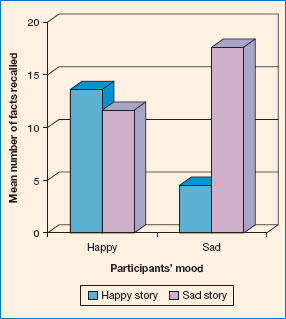
Figure 12.3 Mood congruent memory.
Source: data from Bower (1981).
Interestingly, work on MCM has alerted us to the finding that healthy individuals, in no particular mood, seem to have a positive and potentially adaptive bias towards memory for positive information; most of us are inclined to recall more positive than negative information and events. Some suggest that this helps us to keep a positive outlook on life, in the face of all the problems it throws at us. It is as if we are looking at the world through rose-coloured glasses. It has also sparked a whole field of research into the effects of emotional disorders on cognitive processing, such as the relationship between clinical depression and memory processes, which we turn to next as an example of the application of MCM to real-world issues.
One framework for understanding MCM effects is the ‘encoding specificity principle’ outlined by Tulving and Thomson (1973). This principle states that memory for information will be best when information available at encoding matches that at retrieval. Tulving and Thomson first studied this using words, finding that the words that did not need to be recalled but were present at encoding facilitated memory for the to-be-remembered words when present at retrieval. This idea can be extended to include all kinds of contextual information including emotion. If there is a match between emotional context at encoding and retrieval (for example, mood or other emotional information), memory should be enhanced compared with when there is no match. Applying this to the MCM results shown in Figure 12.3 suggests that if participants’ mood were to be happy at both encoding and retrieval (a matching emotional context), or if other positive information was present in the environment at the time of retrieval of the happy story, this principle can be used to account for the effects observed.
DEPRESSION AND MCM
In contrast to healthy people, individuals with clinical depression, and those who are not diagnosed but still report feeling constantly low in mood (subclinical depression), show MCM effects in the opposite direction, recalling more negative information (one example of a cognitive bias favouring negative material). This is not surprising if you think about it. These individuals already have a low, negative mood, thus the phenomenon of MCM (see Figure 12.3) would predict that they should be better at recalling information that matches this mood. Many different types of experiments have been used to identify and verify this finding. Some of the earliest studies examined recall of autobiographical memories. Findings suggest that individuals with depression will look back on their lives to date and see a preponderance of unhappy life events and sad moments. One possible criticism of these autobiographical findings is that perhaps individuals with depression really have experienced more negative events in their lives to date - and indeed this is may be why they are now depressed (rather than having had similar experiences to healthy controls, but then remembering more of the bad things).
While it is impossible to rule out this alternative explanation when conducting naturalistic experiments, an alternative approach is to use laboratory experiments where the researcher can control more precisely the amount and type of information encoded before testing participants’ recall of this information. Doing this means that both groups, healthy participants and depressed individuals, have access to exactly the same information, and this implies that any bias must truly reflect a recall phenomenon rather than different experiences or patterns of encoding. Experiments of this type have been conducted using stimuli such as positive and negative word lists, self-descriptive adjectives, sentences and whole passages of text. The emotional aspect in the task is the pleasantness/unpleasantness of the stimuli presented and encoded, which is the independent variable. The cognitive bias measure, the dependent variable, is how many words of each type are recalled in a memory test. It turns out that, using these more controlled conditions, findings still show that healthy controls show a positive memory bias (i.e. remember more positive than negative stimuli), while individuals with clinical or subclinical depression have a negative memory bias (i.e. remember more of the negative words in comparison to the controls). The effect appears to be stronger when participants are aware of the relationship between their mood and the material; and, not surprisingly, when the negative nature of the material is stronger.
The finding of negative memory bias in depression is of great interest. This is because it has been suggested that negative memory bias may contribute to keeping someone in a depressed mood and, further, that if we can change this bias, that might help the mood to lift and alleviate the clinical disorder. Teasdale (1988) first proposed and developed this theory, which is represented in Figure 12.4.
Figure 12.4 reflects the suggestion that depression involves a bias towards recalling more negative information, which means that the patient’s world seems more filled with negative things than is really the case. This in turn makes them feel even more depressed. You can see that a vicious circle could be set up, where the memory bias contributes to the mood, which enhances the memory bias (via MCM) and so on. Teasdale and others have spent many years devising methods of breaking this cycle and coming up with new cognitive treatments for depression, the latest being a therapy called mindfulness-based cognitive therapy (Segal et al., 2002).
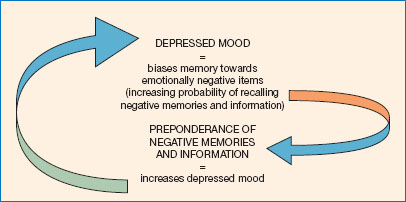
Figure 12.4 Teasdale’s theory of negative memory bias in depression.
Source: adapted from Teasdale (1988).
It is interesting to note that the MCM effect does not appear to occur in anxiety or the anxiety disorders. While there are occasional reports of memory biases associated with anxiety, most researchers who have looked for this, or compared anxiety and depression, have not found any clear evidence of memory biases in anxiety.
12.4 ATTENTION AND EMOTION
In the same way that memory for emotional material can be biased in a direction consistent with one’s mood, so can attention. As with memory, so-called ‘attention biases’ are central to our understanding and treatment of psychological disorders, especially anxiety disorders. A classic example of an attention bias is the ‘emotional Stroop’. In the standard Stroop task (Stroop, 1935), participants are asked to name out loud, as fast as they can, the colour of the ink in which colour words (red, blue etc.) are written. When the ink colour is different from the meaning of the word itself (e.g. ‘blue’ written in red ink), participants are slowed down compared with stimuli where the word meaning and ink colour are the same (e.g. ‘blue’ written in blue ink). The emotional Stroop differs from this procedure in that, instead of colour words, emotional (e.g. ‘fearful’, ‘cancer’, ‘jealous’) and neutral (e.g. ‘corridor’, ‘forest’, ‘suitable’) words are used, still printed in different colours. When the emotional Stroop is given, for example, to high trait anxious individuals, the interference from words relevant to anxiety (such as the examples above) is usually greater than that from the neutral words, compared with the same difference when observed in non-anxious individuals. As performance on the Stroop task is generally taken to be a measure of attention towards the word meanings (although the precise mechanisms behind the effect are still not fully understood), this is an example of an anxiety-related attentional bias.
In an attempt to demonstrate more clearly the nature of this attentional bias, MacLeod et al. (1986) published a now classic paper using an innovative new method of testing attention allocation. An example of a modern version of their task, now known variously as the ‘dot probe’, ‘attentional probe’ or ‘visual probe’ task, is shown in Figure 12.5.
The task is to identify a probe (so called because it is probing where attention is located) as rapidly as possible (in the figure the probe is the letter E or F and participants must press the corresponding key to identify which letter they see). As you can see, before the probe a pair of word stimuli is displayed, one relevant to anxiety (or whatever mood or disorder is being studied) and one neutral. If a participant is consistently faster in identifying the probe when ever it appears where the anxiety-related word previously was, we can reasonably assume that participants must have been attending to that word as opposed to the neutral word. Some typical results are shown in Figure 12.6.
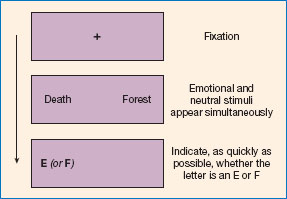
Figure 12.5 A typical trial from an attention probe task.
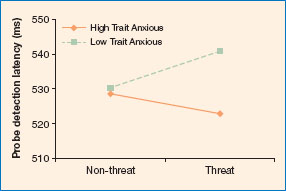
Figure 12.6 Typical results from an attention probe task.
Source: based on Yiend and Mathews (2001).
The figure shows that low trait anxious (but not high trait anxious) participants were faster (by about 10 milliseconds) when probes replaced the non-threat words, rather than the threat words (another example of a healthy ‘positive bias’). High trait anxious participants were the other way round - slightly faster for probes appearing where threat words had been than for probes appearing where neutral words had been. This suggests that high trait anxious individuals allocate their attention to threat words rather than to neutral words, whereas low trait anxious individuals do the opposite. Thus, consistent with the emotional Stroop results, we observe an attentional bias for negative information (in this case, threat) associated with high levels of trait anxiety. The original results of MacLeod and colleagues sparked decades of research, which continues to this day, into this so-called anxiety-related attentional bias for threat. We now know that the bias is seen with many different types of material, including words, pictures and faces, but is most prominent when the material matches the current concerns of the individual. For example, snake phobics will show a stronger attentional bias towards pictures of snakes than towards pictures of snarling dogs.
Most people have a bias to attend to things that match their special interests (for example, bird watchers will attend to bird-like stimuli, in preference to non-bird-like stimuli). Temporary biases are also common, and can, for instance, occur when you have acquired something new, such as a new car. For a while you may find yourself noticing many examples of this same model (and perhaps wonder why there are suddenly so many similar cars on the road!), which previously you ignored. It seems that attentional biases can operate towards any material or information that has a particular relevance (or ‘salience’) to the individual concerned. Remember that the definition of a cognitive bias given earlier allows for this (the tendency for the information-processing system to consistently favour stimulus material of a specific content; Savulich et al., 2012).
However, most research has been conducted within the realm of clinical disorders, because psychologists believe that attentional biases (and indeed cognitive biases generally) may be key to understanding and treating these disorders.
CLINICAL ANXIETY AND ATTENTIONAL BIAS
Attentional bias has been demonstrated in patients suffering a variety of anxiety disorders, including those with phobias, generalised anxiety and post-traumatic stress disorder. In fact it is not only clinical disorders that are associated with attentional biases. Mathews (1990) proposed that a vicious cycle (similar to that shown in Figure 12.4 related to depression and memory bias) could operate to maintain anxious mood and symptoms and that attention bias may therefore be maintaining clinical anxiety disorders. Imagine that your anxiety makes you pick out and pay more attention to potential threats in the environment. It would then seem as if your surroundings were full of threats and this would, unsurprisingly, make you feel more anxious, which would perpetuate your attentional bias and so on. You would end up in a hyper-vigilant state, anxious about everything most of the time. This is the plight of people suffering from generalised anxiety disorder and many other anxiety disorders. As another example, think of someone who is quite afraid of spiders. They may well recognise this characteristic negative attentional bias in themselves. Almost invariably such a person will notice any spider, or spider-like blob, in the surroundings well before their non-phobic companions. Therefore clinical psychologists believe that attentional biases contribute to maintaining these disorders, and, consistent with this, experiments show that negative attentional biases resolve after recovery.
If biases are no longer present after recovery, it could be because they were, in part, sustaining the disorder, as we have suggested. However, it could instead be that the symptoms were causing the bias and once symptoms are treated the bias disappears as a result. In other words, a question arises about the direction in which causality is operating when we observe the co-occurrence of attentional bias and psychological disorder. Mathews and MacLeod (2002) wanted an answer to this question and constructed a more decisive test of whether an attentional bias causes, or was caused by, anxiety (or both). They devised a method of creating (or ‘inducing’) a positive or negative bias in healthy volunteers using customised training procedures. Once a bias had been induced, they then measured the effects on anxiety by investigating how participants responded to a stressful event (and later studies have measured a wide range of outcomes, including clinical symptoms). Typical results are shown in Figure 12.7.
Figure 12.7 illustrates that, before the training procedures (‘pre-training’), both groups responded to the stressful event (watching mildly distressing video clips) by showing an increase in their self-reported state anxiety levels, as you might expect. However, after training (‘post-training’), the two groups differed in their response to watching another, similar, distressing video. Those who had received a negative bias induction (the ‘attend negative’ group) showed the same pattern as before: an increase in their anxiety level after watching the clips. In contrast, those who had received the positive bias induction (the ‘attend neutral’ group) were now much better able to cope with watching the videos and actually showed a drop in their anxiety levels. These results, and others like them, show that reducing a negative attentional bias has a protective effect and increases resilience to stress. The results also confirm that attentional bias has a causal effect on anxiety levels, because directly reducing (or increasing) negative attentional bias reduces (or increases) anxiety levels. It will come as no surprise that these training bias methods have since been developed into new techniques for treating a range of psychological disorders, including the anxiety disorders, and we return to this in detail in Section 12.6.
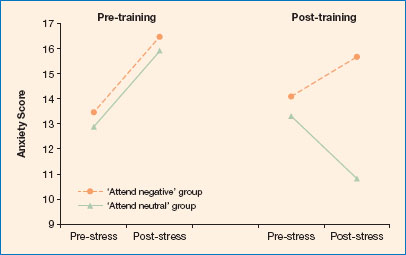
Figure 12.7 Typical results from a stress test given before and after attentional bias training.
Source: adapted from Mathews and MacLeod (2002).
Another similarity between attentional bias and the memory biases we discussed earlier is the performance of healthy, non-anxious participants. As with memory bias, it seems that most of us have an adaptive or protective bias, in the opposite direction to that of individuals with clinical anxiety disorders. Looking again at Figure 12.6, it is clear that the low trait anxious group are faster in neutral areas than in threat areas, and this pattern has been replicated many times. This means that these participants are actively avoiding attending to mildly negative information; they are avoiding processing mild negativity. This active avoidance of minor, insignificant threats would be adaptive in today’s world, and probably enhances our well-being by preventing an unnecessary continuous hyper-vigilant state.
In the case of depression it has proved hard to find evidence of attentional biases, although some researchers have succeeded when the presentation time of the material that is being attended is made very long (for example several seconds, rather than the more usual 500 ms or less). It is thought that this is because biases occur at later stages of processing in depression than in anxiety. Some experts have argued that there may be a double dissociation between anxiety and depression, with anxiety associated with early, automatic, biases in attention, in contrast to depression which is associated with later, strategic biases in memory.
12.5 INTERPRETATION AND EMOTION
Interpretation is another cognitive process known to be influenced by emotion. If you see a word such as ‘batter’, do you think of pancakes or do you think of an assault on an innocent victim? It is surprising how many situations in life can be ambiguous and therefore open to biases of interpretation. In this section we shall consider interpretation of emotionally ambiguous information.
The earliest work on interpretation and emotion used homophones. These are words such as ‘pane’ and ‘pain’ or ‘die’ and ‘dye’, which sound the same but have different spellings associated with different meanings. Eysenck et al. (1987) asked both high and low trait anxious individuals to write down the homophones as they heard them. All the homophones had both a negative and a positive or neutral meaning. This simple technique revealed which interpretation had been made, according to the spelling participants chose. The researchers found that participants with higher levels of trait anxiety produced more threat spellings than those with lower trait anxiety. These results suggested that trait anxiety was linked to a tendency to assume the negative interpretation of an emotionally ambiguous stimulus; a negative interpretation bias. One problem with this research method is that it is possible that participants were aware of, and had access to, both spellings, but just chose to write down the negative one. This matters because, if true, it would mean that there was no bias in the actual interpretation of the words - both interpretations were made. Instead, the bias would be at the stage of making the response, which then says little about the cognitive processing involved in making interpretations.
Figure 12.8 Emotionally ambiguous information can be interpreted either positively or negatively.
Source: copyright Trueffelpix/Shutterstock.com.
Later work used alternative methods to avoid this and other problems. In a classic study, Richards and French (1992) used homographs instead of homophones. These are words that have dual meanings, despite having the same spelling, such as ‘batter’ (cooking or assault?), ‘punch’ (drink or boxing?) and ‘stalk’ (flower or follow?). They used these words in a priming experiment involving a lexical decision task. Lexical decision involves identifying, as rapidly as possible, whether the second of two sequentially presented items is a real word or a meaningless letter string (a non-word). From the participant’s point of view, the first item that appears is just to be ignored. However, this first word is actually a prime. If the prime is related in meaning to the second word (the target), as in cat-dog or nurse-doctor, lexical decisions are faster compared with when primes and targets bear no semantic relation (e.g. cat-doctor, nurse-dog). Richards and French used this logic to infer how participants interpreted the homograph primes. For example, if lexical decisions for trials such as batter-assault were faster than for trials such as batter-pancake, this would imply that the participant interpreted batter as ‘assault’ rather than ‘pancake’. The results of the Richards and French study, as well as other similar studies, suggest that high-anxious participants show a negative bias in interpretation - that is, there is a greater priming effect for target words related to the negative meaning of the homograph than the neutral meaning. For non-anxious participants there is, once again, a positive bias favouring the more positive or non-threatening meaning.
Other studies have extended this research by using ambiguous sentences or longer passages of text, for example:
‘The doctor examined little Emily’s growth’ (her height or her tumour?)
‘The two men watched as the chest was opened’ (a gruesome operation or an exciting find?)
‘Your friend asks you to give a speech at her wedding reception. You prepare some remarks and when the time comes, get to your feet. As you speak, you notice some people in the audience start to laugh’ (appreciatively, or rudely?)
Biases in interpretation are present in healthy people, who generally assume the positive meaning when presented with ambiguity. In contrast, individuals with anxiety and depressive disorders lack this positivity effect, and sometimes show a clear negative interpretation bias. It appears that, as we have seen with other cognitive biases, ‘looking on the bright side’ and assuming a positive meaning where things are uncertain has a protective value and helps maintain health and well-being.
The wider concept of protective processing styles has been described formally in a theory known as attribution theory. Research shows that we attribute good things internally, to ourselves and within our control, whereas bad things we attribute externally, to others, or to circumstances. This reflects a tendency to accept the credit for good outcomes and blame something or someone else for bad outcomes. For example, if you are late for an important meeting or fail your driving test, you might say ‘I’m terribly sorry but the train times have changed and I couldn’t help being late’, or ‘I had such an unreasonable examiner’, or ‘My instructor gave me inadequate preparation’; if you are early or on time, or pass your test first time, you might well congratulate yourself for your efficient organisation and planning, or your excellent driving skills. Closely related to interpretation biases, these kinds of inference are known asself-serving attribution biases. Although self-serving biases might seem (and perhaps are) an irrational way of thinking, the evidence repeatedly supports their existence and, as with other positive biases, they may have protective properties. Moreover, in emotional disorders, particularly in depression or anxiety, we know that this self-serving bias can be lost or even reversed. Such people might think passing the driving test was just luck, or the examiner being lenient, whereas failing was yet more evidence of their own worthlessness and lack of skill. In some situations it can be shown that by lacking the positive bias the depressed person’s attribution of their own performance can be more accurate than for non-depressed controls, so-called ‘depressive realism’. However, the notion of depressive realism is very controversial. For example, a recent meta-analysis (Moore and Fresco, 2012) found that both depressed and non-depressed individuals exhibited a positive bias, although this was greater in the non-depressed individuals. It is worth noting also that, although the various positive biases that we have described are thought to be quite normal, and have protective qualities (such as helping to maintain good mood and a positive self-image), it is equally true that, taken to their limits, they could become maladaptive (for example, leading to mania or grandiosity).
12.6 COGNITIVE BIAS INTERVENTIONS FOR PSYCHOLOGICAL DISORDERS
In this section we consider different therapies and techniques that have been used or are being developed to change the relationship between cognition and emotion, specifically targeting cognitive biases. As we saw earlier, negative biases in memory, attention and interpretation are all associated with various clinical psychological disorders. Psychological therapies often attempt to ameliorate these biases using client-therapist interaction.
COGNITIVE BEHAVIOUR THERAPY AND BIASED COGNITION
In CBT, the therapist explains to the patient the nature of the relationship between their thoughts (cognitions), their feelings and symptoms (emotions) and their behaviours, using a diagram something like Figure 12.9.

Figure 12.9 The basis of cognitive behaviour therapy.
Source: copyright: arka38/Shutterstock.com.
The therapist may help the patient to map their own personal experience onto a similar diagram so that it becomes more relevant to their particular situation. Therapists often make what is known as a ‘formulation’ based on what the patient describes of their difficulties. This is essentially a summary of the presenting problems, a specification of what psychological processes (such as cognitive biases) are contributing to and maintaining the disorder and how they are doing so, and finally a plan for treatment. Therapy then progresses, often using something called ‘Socratic questioning’, which is a kind of questioning that gets the patient to ask and answer their own questions and draws out answers from the patient, rather than the therapist providing the answers. This is thought to promote patient engagement. Frequently therapy also involves some behavioural observations and tasks, as well as ‘homework’, which the patient completes on their own. CBT is a relatively lengthy process that generally spans a number of treatment sessions (typically eight to twelve). During these interactions with the therapist, among other things, the negative cognitive biases in memory, attention and interpretation are identified and addressed with the patient. Treatment frequently includes exposing patients to examples of their particular concerns and encouraging them to reinterpret situations or events in their lives, and re-evaluate memories of past events. The effectiveness of CBT treatment programmes, particularly in both ameliorating symptoms and reducing or eliminating cognitive biases, has been evident for some time (e.g. Mathews et al., 1995).
COGNITIVE BIAS MODIFICATION
We started this chapter looking at cognitive appraisals and how they can influence our emotional responses. We have now come full circle. After considering the various ways in which emotion states, traits and emotional information can all influence, or bias, cognitive processing, we now turn the tables back again to consider what researchers have done to directly manipulate these cognitive biases in an attempt to improve the plight of individuals with psychological disorders. Cognitive bias modification (CBM) techniques are recently developed treatments for psychological disorders which have arisen directly from the laboratory studies used to measure naturally occurring cognitive biases that were described earlier. CBM aims to modify cognitive biases more directly and in a relatively shorter space of time than traditional therapist-led psychological interventions. No therapist is required because the patient can complete CBM independently using just a computer program. CBM is an adaptation of the experimental methods previously utilised to establish the existence of cognitive biases. In this section we will consider two of the most popular varieties of CBM, CBM for attention (CBM-A) and CBM for interpretation (CBM-I).
As you will recall from Section 12.4, attentional bias has generally been measured by probing threat and non-threat locations (see Figure 12.5). When naturally occurring biases are measured, researchers probe each location an equal number of times. CBM-A aims to induce a bias by designing the task such that participants need to attend more to one or other location. For example, for a positive attentional training, the target letters shown in Figure 12.5 would almost always appear in the location previously occupied by a non-threat letter, so that participants must attend away from the negative (threat) information in order to perform the task. After many such trials, participants learn to avoid threat and a ‘positive’ cognitive bias in attention has been created (‘induced’). This kind of procedure is known to work more effectively if participants are aware of the need to attend away from threat, but it is not essential that they know. Researchers demonstrate that a bias away from threat has been induced by presenting new material (e.g. word pairs), but now presenting probes randomly in both locations. As with the original test task described in Section 12.4, if a bias away from negative information has been induced, participants should be faster to identify probes appearing in the location of non-threat words compared with probes replacing threat words.
There has been an explosion of research on CBM-A since MacLeod and colleagues’ initial study (MacLeod et al., 2002). Although some studies are aimed at understanding more about the mechanisms at work, many are directly reporting the use of CBM-A as a treatment for clinical disorders. To pick one example, Amir and colleagues (2009) implemented an eight-session CBM-A programme, designed to reduce attentional bias towards threat and decrease anxiety symptoms, in a sample of individuals with generalised anxiety disorder (GAD). Their method was as described above, using a modified attentional probe task and training participants to attend to non-threatening words on 66 per cent of trials and then testing training-congruent effects on a new set of materials. Self-report and interview measures of GAD showed that training was effective in reducing anxiety symptoms.
COGNITIVE BIAS MODIFICATION OF INTERPRETATION (CBM-I)
CBM-I techniques attempt to induce a cognitive bias in the interpretation of emotionally ambiguous information. As with CBM-A, these methods use adaptations of the tasks normally used to measure naturally occurring biases in interpretation. The adaptation involves presenting the ambiguous information but then instead of letting participants make their own spontaneous interpretation, a cleverly designed task is used to systematically constrain the interpretation to be either negative or positive according to the direction of training. The two main methods used to date correspond to the tasks described previously in Section 12.5 and involve either homographs or passages of ambiguous text.
In the homograph method, first used by Grey and Mathews (2000), participants are repeatedly trained to interpret the threatening meanings of homographs by presenting the ambiguous word followed by the positive associate that participants must complete by entering the first missing letter (e.g. batter: p-nc-ke, pancake or arms: l-s, legs). The word completion task ensures that participants must access the positive meaning of the homograph in order to help them figure out the incomplete word. Positive homograph training reduces an individual’s vulnerability to stress; compared to their negative trained counterparts, those receiving positive training are less distressed by difficult events (such as trying to solve an impossible anagram task or watching stressful videos). Later research has shown that active engagement in processing the desired meaning enhances these beneficial mood effects of training.
The CBM-I method using ambiguous text is more complex, but has, to date, been used more widely than the homograph method. It is illustrated with examples in Figure 12.10. First described by Mathews and Mackintosh (2000), it uses ambiguous passages of text to train participants in making either a positive or negative interpretation of that text. For example, the ambiguous scenario, ‘as you finish your presentation your employer looks up…’, would be given either a positive (… approvingly) or negative (… disapprovingly) outcome by continuing the passage so that the designated meaning becomes clear. To check whether a bias has been created, participants are later given new ambiguous passages and researchers measure how this material is interpreted.
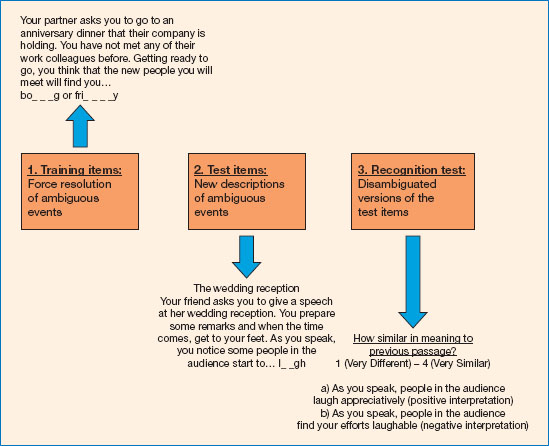
Figure 12.10 Cognitive bias modification for interpretation (CBM-I) using ambiguous passages (e.g. Yiend et al., 2005).
CBM-I using the ambiguous text method has shown effects which are proving useful for the treatment of clinical disorders. The interpretative biases created with this technique have been subjected to various types of laboratory testing to examine their robustness. For example, one study showed that the biases created remain for a day without further training (Yiend et al., 2005), and another suggested that the positive biases that are induced can survive various environmental and contextual changes, which is important if they are to have use in real-world settings (Mackintosh et al., 2006). More relevant to clinical disorders, positive CBM-I was found to produce lasting reductions in trait anxiety levels in one study (Mathews et al., 2007) and to reduce participants’ distress when watching an unpleasant video in another study (Hoppitt et al., 2010). Given these encouraging laboratory findings, it is perhaps not surprising that this method of training away negative biases has been applied to quite a wide range of anxiety and depressive disorders.
However, not all CBM studies have shown good results and the findings of meta-analyses are mixed. In one meta-analysis, Hallion and Ruscio (2011) conclude that multi-session treatments using CBM-I show promise for use as a new psychological intervention. In another, Cristea and colleagues (2015) concluded that most results did not show significant benefit when CBM was used with patients.
TRAINING MEMORY BIAS
Far less research has been done on applications of memory bias research for the clinic, than on the other biases. However, in one recent development, Joormann and colleagues (2009) used suppression training in individuals with major depressive disorder (MDD) to induce forgetting of negative information. Depressed and non-depressed participants first learnt to associate neutral cue words with positive and negative target words. Participants in the training condition were then instructed to suppress negative target words by learning to associate positive or negative ‘substitute’ words with the original cue words. Researchers found that the depressed participants successfully forgot negative words in both the positive and negative substitute conditions, but did not in the unaided (no training) condition. This study demonstrates that suppression training reduces recall of negative information in depressed individuals and that thought substitutes are useful tools for inducing cognitive change. Suppression training is therefore an appropriate method for modifying memory bias.
You can perhaps see how, in real life, this work could be further developed to help to alleviate depression. Following Joorman’s method, we could teach patients to associate an event or memory that was associated with unhelpful negative thoughts with new, alternative, positive information. The new associated positive information should suppress the existing negative associations and produce more helpful thoughts, less likely to trigger the depression.
SUMMARY
✵ Cognitive appraisals (how we think about information) have a significant impact upon emotional responses. Appraisals that ‘play down’ emotional content reduce the emotional response and this can be observed both in lower psychophysiological measures of emotion response and in brain activation patterns.
✵ Emotion states, traits and emotional information all influence the cognitive processes of memory, attention and interpretation. States are feelings of the moment and are transitory; traits are enduring personality characteristics; and emotional information refers to the material or stimuli that carry emotional meaning and upon which cognitive processes operate.
✵ A cognitive bias is the tendency for the information-processing system to consistently favour stimulus material of a specific content.
✵ Mood congruent memory refers to the memory enhancement that occurs when the material being encoded and the mood of the participant at the time of encoding are matched. Individuals with clinical depression show enhanced memory for negative information.
✵ Negative attentional biases, in which threat information is attended to in preference to non-threat, are widespread in subclinical anxiety and clinical anxiety disorders. Attentional biases are commonly measured using the emotional Stroop and visual probe tasks.
✵ Biases in interpretation can be demonstrated using homophones, homographs and ambiguous text. Healthy individuals are positively biased, assuming ‘the glass is half full’, whereas those with psychological disorders tend to be negatively biased and think ‘the glass is half empty’.
✵ Positive cognitive biases contribute to our health and well-being, whereas negative biases exacerbate and maintain psychological disorders.
✵ In cognitive behaviour therapy, therapists work with patients to identify and challenge biased processing.
✵ Cognitive bias modification can be used to reduce unhelpful attention and interpretation biases. These techniques, derived directly from laboratory studies, have been developed into multi-session computerised treatments for use with anxiety disorders and depression.
FURTHER READING
✵ MacLeod, C. (2012). Cognitive bias modification procedures in the management of mental disorders. Current Opinion in Psychiatry, 25. A very readable overview.
✵ MacLeod, C. and A. Mathews (2012). Cognitive bias modification approaches to anxiety. Annual Review of Clinical Psychology, 8, 189-217. Overview of cognitive bias modification as used for anxiety disorders.
✵ Robinson, M. D., Watkins, E. R. and Harmon-Jones, E. (2013). Handbook of cognition and emotion. New York: Guilford Press. Comprehensive coverage of cognition and emotion interactions, including biological and neuroimaging sections, as well as the cognitive aspects covered here.
✵ Wenzel, A. and Rubin, D. C. (eds). (2004). Cognitive methods and their application to clinical research. Washington, DC: APA Books. A practical guide to implementing cognition and emotion experiments in the lab.
✵ Woud, M. L. and Becker, E. S. (2014). Special issue on cognitive bias modification. Cognitive Therapy and Research, 38(2). A selection of examples of the latest primary research into cognitive bias modification and its applications.
✵ Yiend, J. (ed). (2004). Cognition, emotion and psychopathology. Cambridge: Cambridge University Press. Contains chapters on various aspects of cognitive biases and their implications for treatment and understanding of psychological disorders.