Going to Pot: Why the Rush to Legalize Marijuana Is Harming America (2016)
Chapter 2
What Is “Medical Marijuana”?
Nearly half the states in America, plus the District of Columbia, have legalized some form of marijuana use—mostly for “medicinal” purposes. Four states have fully legalized marijuana for “recreational” use. Rather than exhaustively analyze every state’s experience with medical marijuana and what Washington and Colorado have done, we will instead examine some experiences in a few of these states.
A Wide Variety of State-Authorized Medical Marijuana Programs
![]()
Medical marijuana programs vary greatly among the various states that have legalized them. In Colorado and California, for example, thousands of neighborhood dispensaries sell marijuana to anyone with a medical marijuana identification card, which is very easily obtained. In New York, which legalized medical marijuana in 2014, the program is quite different. Only five private companies will be selected to open and operate four dispensaries each. There is a narrow list of eligibility requirements, and any doctor who prescribes marijuana to a patient who does not truly meet the criteria may be charged with a felony. Finally, patients may consume marijuana only through food, oils, pills, or vapors. Smoking marijuana is prohibited.1 It is striking that Colorado has more than five hundred medical marijuana dispensaries with a population of 5.1 million people, while New York has authorized a total of twenty dispensaries with a population of 19.5 million people.
In California, medicinal marijuana was approved in 1996 by about 55 percent of the vote. In 2000, Colorado voters passed a referendum legalizing the use of medical marijuana with approximately 54 percent of the vote. Just to point out that this is not a red state/blue state issue, in 2010, Arizona voters approved their medical marijuana law with just over 50 percent of the vote. In November 2014, voters in Oregon, Alaska, and the District of Columbia voted in favor of outright, recreational legalization. Florida voters rejected a referendum initiative that would have permitted medical marijuana.
Not content with the idea of marijuana use for only medicinal purposes, four states have now gone on to fully legalize recreational use of the drug. This makes the United States only the second nation in the world with fully legalized marijuana use (Uruguay is the other). Not even the Netherlands, notorious as it is for its liberal cannabis policies, formally legalized the sale or use of pot—it merely tolerates it with liberalized laws on enforcement.2 Not so Washington and Colorado, where possession is now, by law, legal. The voters in Colorado enacted their recreational use law in 2012 with 55 percent of the vote; the voters in Washington passed their law the same year, with the same percentage.
The Federal Government Has Abdicated Its Legal Responsibility
![]()
Keep in mind that none of this affects federal law and it is in direct opposition to the federal Controlled Substances Act. Most of us were taught in high school that under the US Constitution, federal law is the supreme law of the land, and states may not violate federal law. Marijuana is allowed to play by a different standard, and even the Obama administration and the Department of Justice have said they will not enforce the federal law against the states that have contravened federal law when it comes to marijuana. Those who took history and civics classes also may remember such concepts as nullification, and that the Civil War put the issue to rest: states may not contravene federal law. Yet nearly half have, with little or no legal consequence. Indeed, the Attorney General of the United States has gone so far as to endorse the states’ thumbing of their noses at the federal law: “I think, so far, I’m cautiously optimistic,” about the laws in Colorado and Washington, said Eric Holder. “But as I indicated to both governors, we will be monitoring the progress of those efforts and if we conclude that they are not being done in an appropriate way, we reserve our rights to file lawsuits.”3 This statement is about two states’ laws that contravene the federal law, which holds that the possession of any amount of marijuana is illegal. The states decided to go another way and the Attorney General is “optimistic.” What message does this send to other states? To law enforcement? To children who used to be taught marijuana was illegal because it was dangerous? The US Attorney General has effectively said “not illegal” and “not so dangerous.” Recall, too, that the President has compared smoking marijuana to smoking tobacco cigarettes, something children and others see being done all the time.
The federal/state conflict informs much of the political debate over marijuana, especially among libertarians on the right. Democrats and the left have not usually been the political precinct in favor of states’ rights (but, again, marijuana changes all the usual rules). We will look at whether the federal laws are, indeed, right. However, for the moment, to answer the question about whether the federal laws are correct, what have been the consequences in California, Washington, Colorado, Arizona, and other states? Early though this experiment in legalization is, we already have some data—and it is not encouraging. On the contrary, it is bad.
“Medical Marijuana for All”—the Medical Marijuana Myth
![]()
Let us start with medical marijuana. Defining medicine through legislative fiat or popular referendum undermines the national drug approval system run by the FDA. The FDA has stringent technical and evidence-based standards that it uses to protect all Americans from dangerous, ineffective, or fraudulent drugs. It puts in place safeguards that include confirmed purity; validated production; tightly controlled manufacturing; known shelf life, microbiology, and efficacy and safety data per dose; documented side-effect profiles; and regular safety updates to keep the FDA apprised. While its approval system may not be perfect, it has shielded us from many unsafe and unacceptable drugs for decades.
As many in the media are wont to say—and many in the culture have adopted such language—one needs a doctor’s prescription to obtain medical marijuana. This is simply untrue. No doctor in America can actually prescribe marijuana: it would violate the acceptable use of his Drug Enforcement Agency-authorized prescription drug pad. What the state laws require are not prescriptions, but recommendation notes or letters from a doctor (or a card issued by the state based on a letter from a doctor). The distinction is important as, again, the culture and children learn from the language that is being used: marijuana is simply not medicine a doctor can prescribe, no matter what it is called. It is not medicine to be found in any pharmacy. Additionally, never in the history of the FDA has there been an authorized form of medicine that is lit up and inhaled. There are doctors who are willing to write notes to patients who can go to dispensaries to buy marijuana cigarettes and brownies, or grow their own. Not pharmacies, but dispensaries and backyards—another important distinction. Unlike medicine, marijuana has no set or controlled dose or strength—that is left up to the users, dispensaries, and growers, many of whom compete for business based on the THC potency of their marijuana. In other words, there is a “race to the top” with dispensaries advertising or promoting higher and higher levels of THC in their product.
How easy is it to obtain such a note, letter, or card? Here’s Will Wooton, a drug and alcohol counselor in Escondido, California:
“First it was almost unbelievable. It was just hard to imagine that you could easily obtain something that can be misused,” Wooton said. “Most of the kids think it’s a joke. In fact, they openly say it’s a get out of jail free card. That is one of the nicknames around high school.”
Wooton said he used to see one to two teenagers a month who used their medical marijuana card as a means to get high. Now he sees more than that every week.
Legally, you must be at least 18 years old to obtain a medical marijuana card, but FOX 5 wanted to find out what else was required, so we decided to follow Wooton’s fellow counselor, Grant Glidewell, as he tried to get a card.
The first clinic we stopped at was in the North County… “The most common thing I hear from kids is that they go in and say they’re anxious and can’t sleep. I’m going to give that a shot and I’m pretty confident that will work,” said Glidewell.
It did work. Less than an hour later, Glidewell walked out of the first clinic with a card to legally smoke pot.
“When I saw the doctor, he smiled and had looked over my questionnaire briefly. He said, ‘You have two of three main symptoms we treat here,’ ” Glidewell said. “He then said that I was going to love marijuana, that he and his wife smoked it and that I was going to have the best sleep of my life.”4
Gone are the days when teenagers wanting to break the law and get high had to plan for days how they would obtain their weed. No more calling friends, and friends of friends, and negotiating prices at covert (often seedy) meeting places. Now, one hour, one pot card. What are the conditions needed to obtain a marijuana recommendation? In California and other states the list is rather long, ranging from cancer to chronic pain. But it can also include any “medical condition that limits the ability of the patient to conduct one or more major life activities.”5 Demand, of course, is high. Thus, so is supply. There seems to be an awful lot of chronic pain out there.
We mean no offense to those with serious illnesses—and we will address this issue further on—but they are an extremely small percentage among the many who are obtaining medical marijuana cards and notes. In Arizona, thirty-four thousand people had medical marijuana cards as of December 2012. Arizona Republic reporter Laurie Roberts says that “3.76 percent use marijuana to ease the symptoms of cancer. Another 1.53 percent suffer from glaucoma while 1.06 percent have AIDS. Meanwhile 89.8 percent—30,203 people—are seeking relief for ‘severe and chronic pain.’ ” Only 13 percent of cardholders are over sixty; “nearly 73 percent of patients are men and the people most likely to seek relief from their pain are 18 to 30 years old.” Roberts was in favor of the law—before she saw its effects, even its early effects. After the law passed and after seeing the numbers above, and the types of people lining up in front of the state’s first dispensary—“not exactly glaucoma-stricken grannies,” as she put it—she changed her mind, calling the law “a charade.” Here is how she opened her column: “I was all set to go along with the charade. All the talk of patients, of care-givers and medicine. But the picture of the teen-age kid holding his skateboard as he came out of Arizona’s first medical marijuana dispensary… Oh come on!”6
Other states show much the same, making one wonder why a recreational law need even be passed when there is a medicinal one. As Maricopa county attorney (aka the district attorney) Bill Montgomery put it, “There’s not a single state with a medical marijuana act or anything similar that hasn’t turned into a recreational use program.”7 In Colorado, for instance, severe pain is the reported condition for 94 percent of medical marijuana users. Three percent have cancer, 1 percent have HIV/AIDS. Seventy-four percent of the patients are male. In California, “fewer than 2 percent of [cardholders] have HIV, glaucoma, multiple sclerosis, or cancer.”8 What of the idea that only adults can use medical marijuana? Two hundred and forty-eight medical marijuana cards have been issued to children under the age of eighteen in Colorado.9
Medical Marijuana Finds Its Way to Children
![]()
Moreover, regardless of what legalizers have said about wanting a system whereby marijuana can be regulated and kept from children, even before Coloradans voted in legalized recreational use of marijuana, their medical marijuana was getting into the hands (and lungs, brains, and hearts) of children. As the Denver Post reported in the summer of 2012, “Nearly three-quarters of teens in two metro-area substance-abuse treatment programs said they have used medical marijuana bought or grown for someone else, according to a new study by researchers at the University of Colorado School of Medicine… In surveys conducted of the teens, researchers asked whether the teens had ever used somebody else’s medical marijuana and, if so, how often. Seventy-four percent of the teens said they had, with a median frequency of 50 times.”10
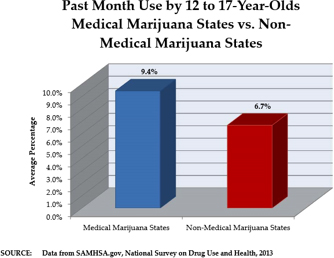
Note, too, for those who like to say marijuana is neither addictive nor harmful, these were teens in substance abuse programs, trying to get sober from marijuana use. In fact, nationwide, one-third of teenagers who live in states with medical marijuana laws get their pot from other people’s “prescriptions.”11 Marijuana usage by twelve-to seventeen-year-olds is dramatically higher in states that have legalized marijuana.
Nationwide, over 70 percent of teens admitted to a substance abuse treatment program claim marijuana as their primary drug of abuse.12 Neither alcohol, tobacco, nor prescription drugs are responsible for over 70 percent of teen substance abuse problems. It is marijuana that has that dubious distinction.
Colorado’s Medical Marijuana Experience
![]()
What have been the consequences of this explosion in medical marijuana use? Colorado provides a dramatic example of how an initially well-intended medical marijuana program can grow out of control with very negative consequences. This earlier medical program was passed by voters in November 2000. It had limits, and between 2001 and 2008, only 5,993 patient applications for identification cards were submitted. Marijuana “caregivers” who provided the medical marijuana were limited to five patients each. Consequently, there were no dispensaries.
In late 2007, a Denver judge struck down the five-patient limit. In 2009, the US Department of Justice issued its guidelines to US Attorneys in those states that had enacted medical marijuana laws. That memorandum advised the US Attorneys to “not focus federal resources in your state on individuals whose actions are in clear and unambiguous compliance with state laws providing for the medical use of marijuana.” The era of medical dispensaries thus began. While much attention has been given to Colorado’s full legalization of recreational marijuana, which was fully implemented with the opening of stores on January 1, 2014, the truth is that the advent of medical marijuana dispensaries and the widespread commercialization of marijuana created de facto legalization in 2009. By the end of 2009, patient applications had grown from a total of just under six thousand in the preceding seven years to an additional thirty-eight thousand in just one year. Also, over 250 medical dispensaries emerged, and were allowed to operate as caregivers, without limitations on the number of patients they could claim. There were 532 licensed dispensaries in Colorado and over 108,000 registered patients by 2012. Not surprisingly, 94 percent of these registered patients qualified for their medical marijuana card by claiming “severe pain.”
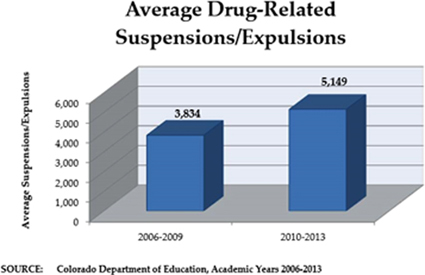
A 2011 study of current marijuana use by twelve-to seventeen-year-olds showed that 10.72 percent of that age group in Colorado used marijuana, compared with the national average usage of 7.04 percent. Also in 2011, the NIDA reported that the average percentage of twelfth graders who had used marijuana in the last thirty days was 22.6 percent. This compared with the Colorado average of 31.2 percent. According to the Colorado Department of Education, the number of drug-related suspensions/expulsions was relatively stable at around 3,800 for each of the academic years ending in 2007, 2008, and 2009. It further reported, however, that those numbers jumped to an average of over 5,100 for the academic years that ended in 2010, 2011, and 2012.
The easy availability of medical marijuana also had consequences for young adults ages eighteen to twenty-five. The National Survey on Drug Use and Health in 2011 showed that for young adults in Colorado, the average past month’s marijuana use was 27.26 percent, compared to the national average of 18.78 percent.
A joint study by the National Institute on Alcohol Abuse and Alcoholism and NIDA, published in 2014, found “an increased number of marijuana-positive Colorado drivers involved in fatal motor vehicle crashes since Colorado’s legalization of medical marijuana in 2009. A similar increase was not seen in the 34 states that did not have medical marijuana laws when this study was conducted.”13 Interestingly, no increase in the number of alcohol-related fatal crashes was found during this time. So much for the argument that “Since alcohol kills more people than marijuana, legalizing marijuana is no big deal.” Nationally, marijuana contributed to nearly three thousand traffic fatalities, 12 percent of traffic deaths, in 2010.14 The National Highway Traffic Safety Administration has found nearly half of fatally injured drivers who tested positive for marijuana were younger than twenty-five.15 As one of the authors of a Columbia University study put it, “If this trend continues, in five or six years non-alcohol drugs will overtake alcohol to become the most common substance involved in deaths related to impaired driving.”16
Just why is it there now are so many fatalities related to alcohol as compared to marijuana? Dr. Nora Volkow of NIDA put it well:
Many more people die of alcohol than all of the illicit drugs together… And it’s not because they are more dangerous or addictive. Not at all—they are less dangerous. It’s because they are legal… The legalization process generates a much greater exposure of people and hence of negative consequences that will emerge. And that’s why I always say, “Can we as a country afford to have a third legal drug? Can we?” We know the costs already on healthcare, we know the costs on accidents, on lost productivity. I let the numbers speak for themselves.17
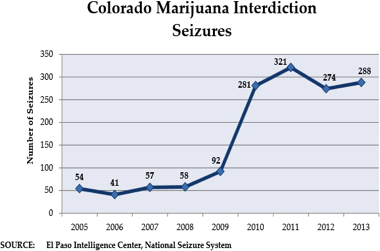
It’s not just teens in states with medical marijuana laws who suffer the consequences. Marijuana, like any commodity, does not stay within its own state. Marijuana bought at dispensaries in Colorado and other states has found its way into states where there are no provisions for medical marijuana. Since the commercialization of medical marijuana, there has been a significant increase in marijuana being diverted from Colorado to other states. The El Paso Intelligence Center (EPIC)18 has established a National Seizure System where seizures of marijuana from Colorado can be reported by police authorities throughout the country. The system is voluntary and by definition, and only includes those shipments that are interdicted, which most interdiction experts estimate represents 10 percent or less of the actual loads of marijuana diverted from Colorado to other states. As can be seen in this chart, the number of seizures has grown dramatically since commercialization in 2009.
Such diversions occur not only by car or truck, but also through the US mail and private package services. The US Postal Inspection Service reported an astounding rise in the seizure of packages containing marijuana that originated in Colorado and were destined for other states.
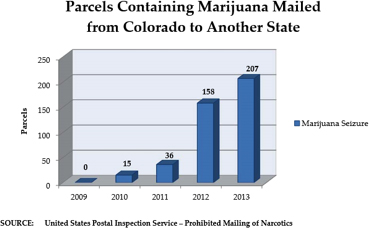
As with the number of police seizures from vehicles, this chart does not capture packages that were mailed and reached, undetected, their intended out-of-state destinations.
Humans are not the only ones impacted by the wider availability of marijuana. “According to a study published in the Journal of Veterinary Emergency and Critical Care in 2012, there has been a fourfold increase in cases of dog poisonings due to marijuana at two Colorado hospitals over the past six years… Two of the reported incidents led to fatalities, including a dog and horse that died after eating marijuana-infused baked goods.”19 Such incidents are not isolated to Colorado. In Arizona, for example, “emergency rooms for pets are seeing more dogs that have eaten marijuana in brownies, cookies, oils and other forms,” according to an article in the Arizona Daily Star. “People come in and their dogs are lethargic, with their eyes rolling in the back of their heads, or they’re unconscious,” Dr. Billy Griswold with Emergency Animal Clinic is quoted as saying.20 Griswold added that over the past few years he has treated at least twenty-four dogs each month that have eaten marijuana. What happens to these dogs? “Unpredictable reactions ranging from depression, staggering and dilated pupils to vomiting, seizures, coma and, in rare cases, death.”21
The Marketing of Medical Marijuana
![]()
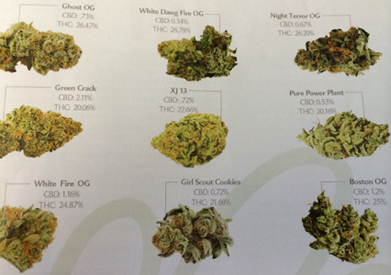
Just how medicinal is this drug for humans? One can easily shop for the nearest or most enticing dispensary on the Web. Take Colorado again, search for “medical marijuana dispensaries” and the Web site WeedMaps gives you dispensaries such as Strawberry Fields Alternative Health, an option in Colorado Springs. This can be replicated in any number of cities. Strawberry Fields promotes “Bubblegum,” “Grape Ape,” “Skywalker OG,” “Voodoo Star,” “Northern Lights,” “Heavy Duty Fruity,” among other flavors. How are these flavors and strains, these so-called medicines, described? Bubblegum: “Very fruity and sweet aroma with a mild hint of bubblegum. Covered in frosted trichomes our bubblegum is a great potent indica. Produces a heavy body high that will have you off your feet and relaxing for hours. Great for patients with multiple sclerosis, bipolar mood swings, muscle relaxer, or for appetite stimulation.” Skywalker: “Sour aroma taste of diesel. Heavy hitting and dream like with a pleasant euphoric high. Long lasting and great for sleep and chronic pain.” Northern Lights: “Strong body high with mellow head buzz. This one is a creeper. Starts off with a mild racy sativa euphoria and works its way down to the body. Putting you in a moderate couch lock stone.” And, one more, Voodoo Star: “This particular strain is one unlike any other. Our most popular and prized strain is Voodoo. The pungent and unique smell of the Voodoo Star will leave you with shock and awe. A delicious taste that stays in your mouth for sometime after being used. Recommended for general relaxation, appetite stimulation, and mild pain/tension relief.” Can you imagine a family physician or neighborhood pharmacist recommending “Voodoo Star”?
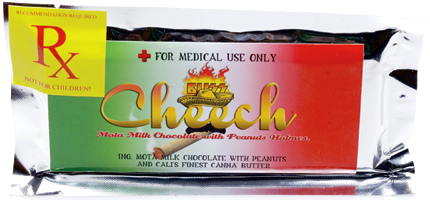
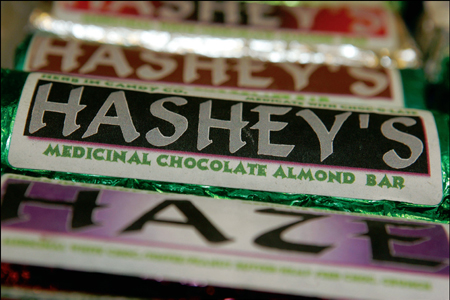
Of course there are all kinds of strains and flavors that sound more like candy for children than medicine for adults. One can find “Grape God,” “Tangerine Haze,” “Pineapple Express,” and “Blueberry” at Kind Therapeutics, also in Colorado Springs. If these strains, and others, sound like the kinds of things children would go for more than adults, there’s a reason for that, just as there is a reason we drive by head shops and dispensaries that have outdoor marketers with signs on the streets at two thirty, three, and three thirty p.m.—not business rush hour, but rush hour for when children leave school. Here are a few pictures of this new medicine:
Bob Berg/Getty


Seth McConnell/Getty

Bob Berg/Getty
Aside from the “Green Crack,”* which is a grotesque appeal to, and conflation of, two dangerous drugs (one more dangerous than the other), one clearly sees the appeal to young people in both the packaging and marketing of this “medicine.”
Thus it should be no surprise to find what JAMA Pediatrics found: according to an article quoting the JAMA study, “When the number of people approved to purchase marijuana for medical use increased sharply in Colorado in 2009, officials witnessed a jump in the number of calls to poison control centers about children inadvertently eating marijuana-laced products, such as brownies, cookies, and candies.”22 The article goes on to say the JAMA researchers, comparing “the proportion of marijuana ingestions by young children who were brought to the emergency room before and after October 2009, when drug enforcement laws regarding medical marijuana use were relaxed,” the JAMA researchers found “no record of children brought to the ER in a large Colorado children’s hospital for marijuana-related poisonings between January 2005 and September 30, 2009… By comparison, they found 14 cases involving marijuana ingestion between October 1, 2009, and December 31, 2011.”23 Eight of those children, none older than twelve, had consumed “medical marijuana,” and all of these had to be admitted to the hospital. While none died, two had to go into intensive care.24
Substance use and abuse begins in the teen years. The average age of first-time marijuana use in the country is 17.9 years for all current users of marijuana.25 The chances that someone will begin using marijuana for the first time after the age of twenty-one are very low. If a dispensary or dealer can get a child hooked, there is a much greater chance of having a client for the long term. This is not a novel strategy: many will recall the societal revulsion caused by tobacco companies marketing to children. Do you remember Joe Camel, a cartoon figure who smoked cigarettes, clearly appealing to youth? He’s not around anymore. Society said our children’s lungs were too important. We repeat, what of our children’s lungs and hearts and brains?
Dr. Nora Volkow, when asked by a columnist recently, “Isn’t tobacco worse than marijuana for teens?,” responded:
Wait a second… Nicotine does not interfere with cognitive ability. So if you are an adolescent and you are smoking marijuana and going to school, it’s going to interfere with your capacity to learn. So what is worse, as an adolescent right now? To have basically something that is jeopardizing your development educationally or to smoke a cigarette that, when you are 60 years of age, is going to lead to impaired pulmonary function and perhaps cancer?… I would argue that you do not want to mess with your cognitive capacity, that that is a very large price to pay.26
She could have mentioned cardiac function and psychosis as well. But the point is made: it makes no sense to say that one substance is worse so we should legalize another unhealthy product. Instead, protecting our children should be guided by concern for the health of all their vital functions.
Just how ubiquitous are these dispensaries selling “Green Crack” and “Voodoo Star” and how much “medicine” is someone allowed to have? In Denver there are more medical marijuana dispensaries than there are Starbucks coffee shops.27 For that matter, there are more dispensaries than liquor stores or licensed pharmacies.28 In Los Angeles, pot stores outnumber the combined total of Starbucks and McDonald’s stores by a ratio of two to one.29Medical marijuana is big business and it is getting bigger.
Every major city has an alternative newspaper, usually a weekly, commonly distributed for free. Its income is based on advertisements. Increasingly the pages of those ads are for medical marijuana dispensaries. Let us look at the way “medicine” is now being promoted in America. Take the Phoenix New Times. It carries two full pages of dispensary ads, right in front of the ads for adult escorts. Here is the text from some of those ads: “New Patients—Get a FREE Gram with the purchase of 1/8th.” “Medical marijuana DELIVERY Now Available.” “Medical Marijuana Evaluations: Walk in Welcome… Get $25.00 Off with this ad.” “ARCH Club: New Patients: Receive Free Gram with the purchase of an 1/8th.” “Herbal Wellness Clinic: Free Gram & Glass Pipe (First Time Patients Only).”30
We are now used to hearing about “Big Tobacco” as a label for companies that sell cigarettes. Why are we not hearing about “Big Marijuana”? Colorado dispensaries reported over $320 million of income in 2013, and in Arizona, the first year medical marijuana was legalized, dispensaries were a $40 million business.31
The Absence of Any Meaningful Regulation of Medical Marijuana
![]()
As for the dose: how much medical marijuana is one allowed to have? In Colorado one is allowed to possess two ounces of marijuana—that is about 120 joints. In Arizona one may buy up to five ounces a month, approximately 300 joints. In some states, such as California, Michigan, and New Mexico, the limit is higher.32 Arizona’s 300 joints a month is approximately ten joints a day. Neither of the authors, who attended college in the 1960s, ever recall any of our acquaintances smoking anywhere near that quantity. Remember, the average THC level today is more than five times greater than it was in those days. In Colorado and Washington State, however, these “limits” are practically useless. In Colorado it is legal to possess up to an ounce of marijuana for “recreational” use, as it is legal to grow your own plants.33 In Washington State one can possess up to an ounce—about sixty joints—but can only grow one’s own marijuana if one has a “medicinal” need.
Our point is this: as serious as the diseases for which marijuana is used are, is it not confounding (and undermining of the case for medical marijuana) that the dispensing and selling of “medical marijuana” are so unregulated, and its packaging so candy-like? We are told about people who have found no relief from spasms or nausea due to very serious illnesses, and then turn to marijuana. They are thus given an unregulated product with varied strengths based on their own preferences, packaged and marketed like this:

This:
Justin Sullivan/Getty
And these:

Of course, each state has a different set of rules, just as each dispensary offers different strains, flavors, and potencies of THC. It is nearly impossible, with such state-by-state variation and voter-approved “medicine,” to take seriously the universal claims of critical need. The “medical marijuana” environment of a wide variety of unregulated products cannot be impressive to medical professionals taking diseases seriously.
The Medical Community and “Medical Marijuana”
![]()
Where is the medical community on the use of marijuana as medicine and who are the doctors who are recommending it? Among the expert organizations, the American Psychiatric Association has said this about marijuana as medicine:
There is no current scientific evidence that marijuana is in any way beneficial for the treatment of any psychiatric disorder. In contrast, current evidence supports, at minimum, a strong association of cannabis use with the onset of psychiatric disorders. Adolescents are particularly vulnerable to harm, given the effects of cannabis on neurological development…
Medical treatment should be evidence-based and determined by professional standards of care; it should not be authorized by ballot initiatives. No medication approved by the FDA is smoked. Marijuana that is dispensed under a state-authorized program is not a specific product with controlled dosages. The buyer has no way of knowing the strength or purity of the product, as cannabis lacks the quality control of FDA-approved medicines.34
The American Medical Association voted last year to reaffirm its official position that “cannabis is a dangerous drug and as such is a public health concern.” The American Society of Addiction Medicine states, “Controlled substances are drugs that have recognized abuse potential. Marijuana is high on that list because it is widely abused and a major cause of drug dependence in the United States and around the world.” Interestingly, ASAM continues:
“Cognitive dissonance” is a term that aptly describes the current approach to “medical marijuana.” Scientists recognize the public health harms of tobacco smoking and urge our young people to refrain from the practice, yet most cannabis consumers use smoking as their preferred delivery mechanism. The practice of medicine is increasingly evidence-based, yet some physicians are willing to consider “recommending” cannabis to their patients, despite the fact that they lack even the most rudimentary information about the material (composition, quality, and dose, and no controlled studies provide information on its benefit and safety of its use in chronic medical conditions). Pharmaceutical companies are responsible for the harms caused by contaminated or otherwise dangerous products and tobacco companies can be held accountable for harms caused by cigarettes, yet, dispensaries distribute cannabis products about which very little is known, including their source. Efforts are being made to stem the epidemic of prescription drug abuse, including FDA-mandated risk management plans required for prescription medications, yet cannabis distribution sites proliferate in many states, virtually without regulation.35
Cancer? The American Cancer Society’s official position is this: “The ACS does not advocate the use of inhaled marijuana or the legalization of marijuana.”36 Glaucoma? The American Ophthalmological Society:
Marijuana cigarettes also contain hundreds of compounds that damage the lungs, and the deleterious effect of chronic, frequent use of marijuana upon the brain is also well established… Unless a well tolerated formulation of a marijuana-related compound with a much longer duration of action is shown in rigorous clinical testing to reduce damage to the optic nerve and preserve vision, there is no scientific basis for use of these agents in the treatment of glaucoma.37
The American Academy of Pediatrics:
The significant neuropharmacologic, cognitive, behavioral, and somatic consequences of acute and long-term marijuana use are well known and include negative effects on short-term memory, concentration, attention span, motivation, and problem solving, which clearly interfere with learning; adverse effects on coordination, judgment, reaction time, and tracking ability, which contribute substantially to unintentional deaths and injuries among adolescents (especially those associated with motor vehicles); and negative health effects with repeated use similar to effects seen with smoking tobacco… The American Academy of Pediatrics opposes the legalization of marijuana.38
So who are the doctors recommending marijuana? Any doctor can recommend it in a state that has legalized its medicinal use—and in many cases the doctors are wholly out of the field of brain or even lung care: they are obstetricians, general practitioners, and doctors in almost every other specialty, including naturopathic medical doctors (not medical doctors or doctors of osteopathy). Some medical marijuana dispensaries, where the doctors practice and recommend on site, even have games and giveaways—ostensibly to entice, who, adults?39
It is worth noting that it is increasingly and tellingly difficult to actually find a psychiatrist to recommend marijuana. As quoted above, the American Psychiatric Association’s official statement cites a strong association of cannabis use with the onset of psychiatric disorders and finds that adolescents are particularly vulnerable to harm.40 As one nationally prominent psychiatrist, Dr. Timothy Jennings, recently put it: “Medical marijuana for the treatment of psychiatric problems is no better than prescribing cigarette smoke to treat lung disease.”41
When Emotion Trumps Science
![]()
Still, we will find doctors who disagree; sometimes they are medical celebrities. One who recently gave credence to the claim of marijuana’s medical benefits is Sanjay Gupta, CNN’s chief medical correspondent. Here is some of what Dr. Gupta wrote in 2009:
I, like many other doctors, am unimpressed with the proposed legislation, which would legalize marijuana irrespective of any medical condition.
Why do I care? As Dr. Nora Volkow, director of NIDA, puts it, “Numerous deleterious health consequences are associated with [marijuana’s] short and long-term use, including the possibility of becoming addicted.”
What are other health consequences? Frequent marijuana use can seriously affect your short-term memory. It can impair your cognitive ability (why do you think people call it dope?) and lead to long-lasting depression or anxiety. While many people smoke marijuana to relax, it can have the opposite effect on frequent users. And smoking anything, whether it’s tobacco or marijuana, can seriously damage your lung tissue.42
In 2013 Dr. Gupta had a change of mind. In fact, he wrote a public “apology” for his erstwhile position. Here is some of his apology:
I apologize because I didn’t look hard enough, until now. I didn’t look far enough. I didn’t review papers from smaller labs in other countries doing some remarkable research, and I was too dismissive of the loud chorus of legitimate patients whose symptoms improved on cannabis.
Still, Dr. Gupta’s article is mostly anecdotal. He tells one persuasive story, for example:
In fact, sometimes marijuana is the only thing that works. Take the case of Charlotte Figi, who I met in Colorado. She started having seizures soon after birth. By age 3, she was having 300 a week, despite being on seven different medications. Medical marijuana has calmed her brain, limiting her seizures to 2 or 3 per month.
I have seen more patients like Charlotte first hand, spent time with them and come to the realization that it is irresponsible not to provide the best care we can as a medical community, care that could involve marijuana.43
Every one of us should be able to sympathize with Charlotte Figi’s plight. We can think of very few who would deny her whatever it is that helps her, and in cases of true medical need, we agree. Set out later in this chapter, we propose a way to legally provide safe and pure medical marijuana. That said, almost every study we have found on the medicinal effects of marijuana is anecdotal. There are many questions about Dr. Gupta’s change of mind that go unanswered. For example, does Dr. Gupta renounce his agreement with Dr. Nora Volkow above? Why doesn’t he address legalization? In his most current piece, he does, however, admit this:
I do want to mention a concern that I think about as a father. Young, developing brains are likely more susceptible to harm from marijuana than adult brains. Some recent studies suggest that regular use in teenage years leads to a permanent decrease in IQ. Other research hints at a possible heightened risk of developing psychosis.
Much in the same way I wouldn’t let my own children drink alcohol, I wouldn’t permit marijuana until they are adults. If they are adamant about trying marijuana, I will urge them to wait until they’re in their mid-20s when their brains are fully developed.44
That is hardly a wholesale endorsement of legalizing marijuana. It fails to take into account the movement of marijuana from a dangerous product to what is now marketed as a healthy and helpful product. It further avoids acknowledgment of the widespread use and abuse of marijuana by the young. Finally, while he writes marijuana should only be available for adults, would Dr. Gupta deny it to Charlotte Figi? She is now seven years old.45Amazingly, there are now marketed strains of marijuana cleverly named after both Charlotte Figi and Dr. Gupta,46 “Charlotte’s Web” and “Gupta Kush.” Going forward, here is the medicine Dr. Gupta can take credit for:

But how do we seriously help the Charlottes of the world? After all, there are a few asterisks on the studies and claims finding “no” medical or therapeutic use, inserted by a handful of experts, perhaps like those cases witnessed by Dr. Gupta. Thus, we propose a modest prescription marijuana protocol.
It is clear that today, the public, in vast numbers, supports some form of “medical marijuana” regimen for those who suffer and claim to need it. Such support runs as high as 85 percent.47 Usually when pollsters ask about this, they refer to a doctor prescribing marijuana for patients who need it. As we know, that is not how medical marijuana works today: “patients” are not regular patients, but rather walk-ins to a “clinic.” The clinic is more of a storefront competing with others for the highest levels of THC with the most attractive or enticing strains and giveaways. “Prescriptions” are not prescriptions at all but “recommendations” and “notes.” There is no real limit to the variety of complaints or perceived illnesses these “patients” seek to alleviate with marijuana; nor are there barriers to the marijuana’s ending up in the hands of adolescents and others wanting it for recreational use. None of this actually has to be the case.
The Scientific Evidence on Marijuana as Medicine
![]()
We recognize what some in the sober and serious medical community have recognized, such as the Institute of Medicine, which, while generally opposing the use of smoked marijuana for medicinal or any other purposes, does recognize that “people have varied responses to medications, and there will likely always be a subpopulation of patients who do not respond well to other medications.”48 The Institute of Medicine goes on to say there is a possibility marijuana use “would be moderately well suited for particular conditions, such as chemotherapy-induced nausea and vomiting and AIDS wasting.”49 Additionally, Drs. Samuel Wilkinson and Deepak Cyril D’Souza of the Yale School of Medicine wrote in the May 2014 Journal of the American Medical Association (JAMA) that “Evidence supporting [marijuana’s] efficacy varies substantially and in general falls short of the standards required for approval of other drugs by the FDA. Some evidence suggests that marijuana may have efficacy in chemotherapy-induced vomiting, cachexia [wasting] in HIV/AIDS patients, spasticity associated with multiple sclerosis, and neuropathic pain.”50 They also go on to write “the evidence for use in other conditions—including post-traumatic stress disorder, glaucoma, Crohn’s disease, and Alzheimer disease—relies largely on testimonials instead of adequately powered, double-blind, placebo-controlled randomized clinical trials.”51
The idea that medical marijuana can be used for a long laundry list of conditions, such as we hear about in states that have approved medical marijuana at the ballot box, is nowhere accepted in serious scientific literature. Indeed, as Wilkinson and D’Souza write, “The many conditions for which medical marijuana is approved have no common etiology, pathophysiology, or phenomenology, raising skepticism about a common mechanism of action.”52 No one medicine has ever been recommended or used for the number of diseases and ailments political proponents of medical marijuana say it is a therapy for. The proponents have turned it into some kind of major miracle drug while, at the same time, the scientific literature finds marijuana either dangerous or of extremely limited use, and often both. However, what of the “subpopulation” of those suffering such things as cachexia, multiple sclerosis spasticity, and vomiting who have found no relief in any other drug or substance? The experts cited above write “some” evidence “suggests” that marijuana “may” have efficacy in three or four circumscribed kinds of cases. There is “a possibility” that marijuana “may” be “moderately well suited” for a few of these conditions. Furthermore, it seems probable that “there will likely always be a subpopulation of patients who do not respond well to other medications.”
FDA-Approved Marijuana Drugs
![]()
What many people do not know is that since 1985, there has been a prescription form of synthetic marijuana, known as Marinol or dronabinol. Marinol, while man-made, contains many of the same properties as regular, smoked marijuana but is manufactured in a gelatin capsule in various doses. It is not smoked or put into candy bars or brownies. Neither, however, is it used or recommended for, or has it been found to be efficacious for, the full laundry list of conditions those who argue for “medical marijuana” claim smoked marijuana can alleviate. It is primarily prescribed “for treating nausea and vomiting associated with cancer chemotherapy and for treating anorexia associated with weight loss in patients with AIDS.”53 Does Marinol actually work? Again, as with any medicine, there will be a subpopulation that does not respond to its effects. And, because it is swallowed in a capsule, the time it takes to affect nausea or vomiting in a patient is going to vary, and take longer to work than the immediate hit smoked marijuana provides. Inhaled marijuana’s effects can begin to work in about fifteen seconds, whereas a dose of Marinol may take upwards of an hour and a half. We would urge those who find no relief for the conditions they suffer from, and want to try smoked or candied marijuana, to first seek Marinol. We further understand that not every medicine is effective in all cases for all patients.
We also are as interested as anyone in this debate as to the conclusions the FDA reaches on Sativex, a spray version of cannabis extract. Sativex, manufactured in Great Britain, has been used in other countries and has been shown to be effective in treating spasticity and some forms of pain. As with Marinol, its method of delivery and manufacture allows for a controlled dose. Although the FDA has fast-tracked its approval process in the United States, as of this writing, it is still being tested. If Sativex is ultimately approved, and joins Marinol as a form of prescription relief, it will be interesting to see if the demands for inhaled or candied marijuana remain unchanged. In other words, the scientific, medical, and government authorizing communities are taking the demands for relief found in marijuana seriously, by putting the active ingredient into standardized pill and aerosol forms. Should Sativex join Marinol, one might think the clamor for smoked and candied marijuana, which has no controlled dosage and no quality control on content or safety and is pretty much self-administered through a loose process of recommendations by naturopathic doctors and chiropractors and a very small minority of the medical community, would subside or be rendered nearly irrelevant.
We shall see. Our best guess is that if Sativex is approved, there will actually be little or no reduction in sales of “medical marijuana” by the numerous dispensaries enjoying economic gain. This is because the vast majority of those purchases have nothing to do with medication and are entirely geared toward getting high from the smoked and eaten product rather than obtaining relief from the regimented and truly prescribed medicinal form of it. The purchasers are not so much patients as they are recreational users.
Prescription Marijuana—A Modest Proposal
![]()
Still, we recognize that Marinol or Sativex may not be efficacious in all patients—no drug is. (It is an interesting side note that this admission about lack of 100 percent efficacy in legal drugs is almost never made by proponents of smoked or eaten marijuana about their products. Not only is the efficacy of smoked and eaten marijuana vouched for with nearly 100 percent conviction, the list of ailments that smoked and eaten marijuana arguably treats is ever-expanding.) Thus, we propose a medical and political solution. It would require a rigorously monitored process by which these real patients (e.g., those suffering from cachexia and spasticity who have found no relief in other, approved drugs) can obtain what they need. This would be somewhat similar to a program the FDA ran from 1978 until 1992, whereby a small number of patients were given marijuana cigarettes with a known and consistent THC level. Participation in this program had to be approved by the National Institutes of Health, the FDA, and the DEA. Modeled on that Compassionate Investigational New Drug program, we propose the following:
Medical marijuana could be used for certain patients according to the following criteria:
1. A patient can participate in this program only with a special waiver from a physician who attests that other medications have been tried and failed to relieve the condition.
2. The program is limited to those who suffer from those few conditions for which the Institute of Medicine has found some evidence that smoked marijuana may be helpful when other medications have not.
3. Both the patient and physician must sign a formal statement, under penalty of federal perjury charges, attesting to the use of only this marijuana, by only this patient, for only this condition.
4. The patient must also sign a waiver of understanding that the use of marijuana can lead to any number of adverse side effects, releasing the government from any potential liability.
5. The physician, aside from facing perjury charges, is subject to loss of his or her medical license for violation of this protocol.
6. The condition must be chronic, that is to say long-term and not temporary.
7. The government-provided marijuana must be at a standardized dose (the Compassionate Investigational New Drug program used a standardized 3.5 percent THC level).
8. The physician must be a specialist in the field of the disease the patient suffers.
9. A hospital pharmacy must fill the prescription the government approved and the doctor certified.
10. The patient must regularly receive prescriptions based on regular reviews—perhaps weekly or bimonthly—of his or her case by the physician.
A program or set of protocols such as the foregoing could do much to solve the true problems suffering patients now have, while at the same time remove the potential for abuse and diversion to adolescent and other recreational populations. Doctors and scientists would be able to see how efficacious marijuana actually is. There could no longer be any claim that opposition to marijuana is political, as this plan challenges the vast number of people clamoring for legalization for therapeutic purposes. It puts a substance that may be helpful, but has great potential for abuse, exclusively into the hands of doctors and true patients. This proposal, we believe, should and could be embraced by both sides of this debate. We might call this “prescription marijuana.” That would distinguish it from the “medical marijuana” label that has been put on what many see as a bad joke, giving this product and process the seriousness true patients say they need and deserve.*
Such a regimen also would cause the US Attorney General to demand and ensure closure of all medical marijuana facilities based on the enforcement of federal law. Indeed, this program would likely not work if medical marijuana dispensaries continued to operate. At the end of the day, we have taken seriously the medical issues and patient frustration and provided a safe and accessible protocol for the dispensing of a potentially beneficial substance to that small part of the population certain scientific and medical communities suggest may be helped. This is both a political and a medical solution to the debate over “medical marijuana.” In sum, those who truly might benefit from it can get it, almost like any other true medication dispensed by prescription, and those who oppose such a program need to be asked, “Why?”
It is important to recognize the rigor of such a program, just as it was important to have the scientific community test Marinol before it went to market, just as it is important to await the results of the approval process that has now been “fast-tracked” for Sativex. Those researchers and physicians who have published their concerns about smoked or eaten marijuana in such journals as the Journal of the American Medical Association, the New England Journal of Medicine, and elsewhere all caution that medicine—true, therapeutic, safe, and efficacious medicine—is not and cannot be subject to a vote. Medicine, like disease, is serious business. Its recognition, use, deployment, and method of delivery should not be determined by popular demand. We do that with no other medical treatment, not even over-the-counter non-prescription drugs. As doctors Wilkinson and D’Souza put it in the JAMA:
If marijuana is to be used for medical purposes, it should be subjected to the same evidence-based review and regulatory oversight as other medications prescribed by physicians. Potentially therapeutic compounds of marijuana should be purified and tested in randomized, double-blind, placebo- and active-controlled clinical trials. Toward this end, the federal government should actively support research examining marijuana’s potentially therapeutic compounds. These compounds should be approved by the FDA (not by popular vote or state legislature), produced according to good manufacturing practice standards, distributed by regulated pharmacies, and dispensed via a conventional and safe route of administration (such as oral pills or inhaled vaporization). Otherwise, states are essentially legalizing recreational marijuana but forcing physicians to act as gatekeepers for those who wish to obtain it.54
Our modest proposal does go one step further, of course. We are willing to try, and have outlined a method to effectuate, a physician-based regimen for inhaled marijuana. It will be interesting to see whether, if this proposal is adopted, the call for dispensaries and unregulated use ceases. We know the dangers of “medicine by vote” from our recent history. Laetrile was that example. Promoted as a cure for cancer, Laetrile was made from apricot and peach pits. It was never approved by the FDA, and many sought it in Mexico and elsewhere. Indeed, some twenty US states voted to approve its use throughout the 1970s,55 but to no therapeutic avail, and several people died of cyanide poisoning as a result of using Laetrile. Most importantly, though, cancer patients suffered, not only from false hopes and promises, but from the distraction of using a quack medicine as an alternative to scientifically researched and recommended standard medicines used to treat cancer. As one British doctor put it, “Testimonials are not science.”56
We believe our proposal can resolve much of the debate, while getting the desired marijuana into the hands of those who may truly need it, just as Dr. Gupta suggests. Still, in the main, we are cautious because the idea that medical marijuana was always about therapeutic medicine, or ever was, is belied by the former executive director of the largest marijuana legalization advocacy organization in America, the National Organization for the Reform of Marijuana Laws (NORML), Richard Cowan. Mr. Cowan is on record and video as saying, “The key is medical access, because once you have hundreds of thousands of people using marijuana under medical supervision, the whole scam is going to be brought up… Then we will get medical, then we will get full legalization.”57 Colorado got the message.