Ebola: How a People's Science Helped End an Epidemic - Paul Richards (2016)
Chapter 4. EBOLA IN RURAL SIERRA LEONE: A TECHNOGRAPHY
This chapter and the next offer an empirical analysis of the Ebola epidemic from the perspective of techniques of the body. They draw on a survey of twenty-six villages in central and eastern Sierra Leone undertaken in December 2014 at the peak of the epidemic. Topics discussed include local understanding of the causes of Ebola, access to treatment, local burial practices, and responses to quarantine and ‘safe burial’. Findings show that villagers had formed their own evidence-based appraisals of links between techniques of the body and Ebola infection. It is also apparent that villagers had very negative views of the safe burial process. The need for this process was not denied, but community members demanded to be trained and equipped to carry it out themselves. Everywhere the call was the same: villagers needed to be able to invest the new techniques of the body to counter Ebola with appropriate social values. Following the argument developed in Chapter 3, a new co-production of body technique and local collective representations was required.
Exploring ‘technique’
An initial requirement is to explain the use of the terms ‘technique’, ‘technology’, ‘technography’ and ‘task group’. ‘Technique’ here refers to skill as an embodied set of social practices directed towards some kind of material or non-material end, with or without the use of tools and machines.
Marcel Mauss suggested regarding the body as our first tool. This may seem strange because technology studies often foreground instruments over the user of the instrument. Mauss’s move is intended to provoke thought.
There is nothing contradictory about referring to the technique of a skilled singer. Human lungs and vocal cords are an embodied instrument. Nor, by referring to the body, or parts of the body, as an instrument, is Mauss retreating from the idea that technique always has a social context.
Social practice - the work of teachers, for example - is crucial in training the voice. To be self-taught is no exception, since the very idea of self-instruction implies pedagogy as a larger frame of reference. If we teach ourselves to sing we simply become teacher and pupil rolled into one.
‘Technology’ is used in the strict sense of ‘knowledge of technique’. Properly, it should always be carefully qualified in terms of the domain of application.
Under the influence of commerce, advertising and journalism the word is often shorn of qualifiers, and used to imply something like ‘our latest product’. When qualifiers are restored - ‘new technology’, ‘advanced technology’, ‘smart technology’ - hidden assumptions become apparent; the implication is that current knowledge of technique is inherently obsolescent, regressive or stupid. This is the language of advertising, and it is unfit for scientific purposes.
Technology is inadequately described unless contextual factors relating to usage are taken into account.1 These contextual factors are inescapably social, and include all aspects of human cooperation, from familial intimacy to industrial division of labour. The centrality of the social in so-called ‘new technology’ is apparent in the now ubiquitous phrase ‘social media’. The smartphone without contacts is not a phone.
‘Technography’ is a neologism, but useful nevertheless, because it immediately suggests a link with the more widely known word ‘ethnography’, used by anthropologists and others to index the detailed description of social processes, often based on directly observed qualitative data, including data derived from participation in, or being trained to perform, a task.
Technography focuses on the detailed description of technique, including descriptions based on the observer’s acquisition of a specific technique, and is thus an important tool to acquire knowledge of technology. A title such as ‘How I taught myself to sing: a technography’ would make perfect sense.
Technography will also, often, provide information about the organization and performance of the ‘task group’. Many techniques involve group effort, and group effort generally involves learning to work as a team. A full description of the task group, and how it is organized, trained and governed, is an essential aspect of technological knowledge. Research on task groups spreads over several fields, from anthropology to management studies. Two classic contributions might be mentioned - by Thomas McFeat and Frederick Brooks.2
Controlling Ebola requires new kinds of task groups to be organized and trained: barrier nursing specialists, safe refuse disposal groups, ambulance crews, safe burial teams. How these are formed and function, and relate to other relevant community groups, notably the family caring unit, should be a focus for reflection by anyone contemplating social mobilization for Ebola prevention.
Organizational style is also an important aspect of the study of task groups, and relates closely to the concerns of Mary Douglas and others with uncovering the ‘elementary forms’ that go towards making institutions work.3
McFeat opens his seminal book on the anthropology of task groups with an instructive story. As a young Canadian soldier, standing on the banks of the Ems river waiting to cross into Germany, in the last days of the Second World War, he saw a strange contraption on the river ahead of him. It was a segment of a Bailey bridge being floated across on pontoons, with four outboard engines strapped to the corners. A sergeant stood in the middle, trying to command the four motormen, in the teeth of a gale. Deafened by the wind, each motorman had his own ideas about when to apply power. The thing went round in circles.
Straight away McFeat realized that this was a boat designed by the army. It followed a parade-ground model of command. If the navy had been in charge, they would have built a lookout, blindfolded the four motormen, and connected them to the commander in the lookout by a system of pull-ropes and bells to issue unmistakable and unambiguous orders. The pontoon bridge section went round in circles because the wrong task group model had been applied.
The same question can be asked about Ebola control. Were new and often hastily improvised task groups for breaking chains of Ebola infection sound, both in regard to biosecurity objectives and also (crucially) in their fit with the local social context? Or did the response bring with it too many unquestioned assumptions on the part of responders about the way biosecure facilities and processes ought to be run in the social and medical conditions with which they were familiar?
The Hewletts report that local negative responses to patient isolation in previous Ebola outbreaks resulted from the use of tarpaulin walls in treatment units. This meant families could not see what was happening. Dark suspicions were formed. Sometimes, distrustful families reclaimed patients, and deadly consequences followed. This information was published in 2007, but still I saw several sites of (now disused) Ebola holding units and community care centres (CCCs) in Sierra Leone with opaque tarpaulin walls. Recurrently, informants complained that the inability to witness what was happening to their loved ones fed dark suspicions, and sometimes resulted in attempted rescues. Design of treatment facilities requires a social understanding of what needs to be witnessed, and why. A more thorough technography of care might support such better understanding.
Going home to be buried
Like McFeat, I begin with an observational vignette.
One day during a period of fieldwork in Mogbuama, a village in Kamajei chiefdom, a friend - an elderly hunter - arrived at my door. He had looked after me with great kindness for a number of years. A leading ‘society’ man, and headman of one of the village’s five quarters, my friend’s main complaint about me was the poor state of my Mende, since there were many things he would have liked to discuss with me more deeply.
He now struggled to explain that he had a daughter whom I had never met because she was married in a chiefdom some miles away, and that news had arrived to say she was sick, and close to death. She had TB. Would I help him by loaning my truck, then garaged at Njala, and drive to a village on the road to Moyamba, to collect the young woman, and bring her home?
Momentarily, I wondered about the advisability of transporting a very sick person on the back of an open truck, along a bone-shaking and dusty track. The last six miles would have to be by hammock, since my vehicle could not cross the two rivers that cut off Mogbuama, in those days, from the national road network. My friend assured me that ‘yes, she must come’, and ‘yes, a hammock party would meet me’ at the point where the footpath to Mogbuama joined the road.
When we arrived at the young woman’s marital home it was already late in the evening. A party was waiting and silently arranged her, wrapped in what seemed to be several thick, locally woven country cloths, as comfortably as they could on the back of the truck, packing themselves and the items they needed around her, to provide shelter as far as possible from the night air. There were only whispered farewells, and few overt signs of the grief the husband’s family must have felt at their loss. I was told to proceed.
We met the hammock team, silently waiting, as arranged. Relays of strong young men would take turns in managing the hammock along a rutted track, taking especial care over a long system of stick bridges carrying them over the braided and treacherous Tibai river, where it finally tumbled over the last step of the escarpment onto the coastal plain. Fortunately it was a moonlit night.
I waited a few moments while the hammock bearers and party of family and sympathizers moved off down the track, their way lit only by a couple of flickering storm lanterns. The procession reminded me of a poem by Robert Bridges, memorably set to music by Gustav Holst, about the funeral procession of a young woman, killed by grief, going to meet her dead lover.4
Hearing the music play in my head as I stood there in the moonlight blocked out for a time an obvious question. Why was this woman going away from her (living) husband to die and be buried at home?
Only much later did I begin to piece together the answer. It was complicated. Probably, there was going to be one last attempt to find a local cure, though, in fact, the young woman died the next day. As important was that she would now be laid to rest by members of her own family (ndehun, in Mende) in family ground. But I did not understand why the evidently distressed, not to say grief-stricken, husband did not play a greater part.
The explanation was that the marriage was one that in local social taxonomy is classed as ‘incomplete’. This means that the promises of gifts and material help a husband and his family make to the family of the woman, before the union is agreed, had only been partly fulfilled. Until these obligations were fully met the man did not have the right to make arrangements to bury his wife. The body belonged to her ndehun. Only if he could afford, there and then, to discharge his obligations could he claim that right.
Behind this belongs a complex web of ideas about marriage, land and ancestral spirits. Landowning groups form alliances by marriage. Marriage, for Mende-speaking people, is a process, not a state. Only death determines whether, truly, you were married. A wife will sometimes answer the question ‘are you married?’ with the response ‘time will tell’. The husband’s obligations to the wife of his family are open ended. They have provided the greatest of all gifts - the means of life itself. This cannot be repaid, so the attempt is never ending.
But there is a ritual moment when enough has been provided, by way of loyalty to the woman’s parents, for the parties to say this person is now truly our in-law; we are now sure he will never abandon our daughter, or us. This is when the marriage can be deemed socially to be complete. At death, the wife will then be buried where her husband chooses.
But going outside this contextual frame potentially stirs anger - the anger of a wife’s family, of a soul not at peace, and of the ancestors. People fear a loss of blessing. The established order of social values has been affronted.
Of course, people also recognize that circumstances dictate that not everything can be done as required. A wife may die far from home and the burial has to be arranged in situ. But in such cases ritual transactions are needed to make reparation. A man can marry his wife after her decease, by offering what was not provided during her lifetime. This will regularize the situation, and thus calm the disturbed social (spiritual) forces. What is done is flexible. But something has to be done. Bodies cannot be dumped, but neither can they be buried where they are not supposed to be. Burial technique - and that includes Ebola ‘safe burial’ - cannot avoid adaptation to the social framework.
Care for the sick and dead
Chapter 5 describes in detail burial technique in rural Sierra Leone. First, some evidence on patterns of care for the sick and dead is presented and discussed.
Field study in Sierra Leone, carried out in December 2014, covered twenty-six villages (see Table 4.1). Selection was purposive. Twenty villages were chosen because they had been studied previously, and baseline data existed. Only one of these villages had experienced an Ebola outbreak, so six more villages with Ebola cases were added to the sample.
Table 4.1 Whether or not to wait before seeking treatment for a sick villager (typical waiting times = 1-3 days)
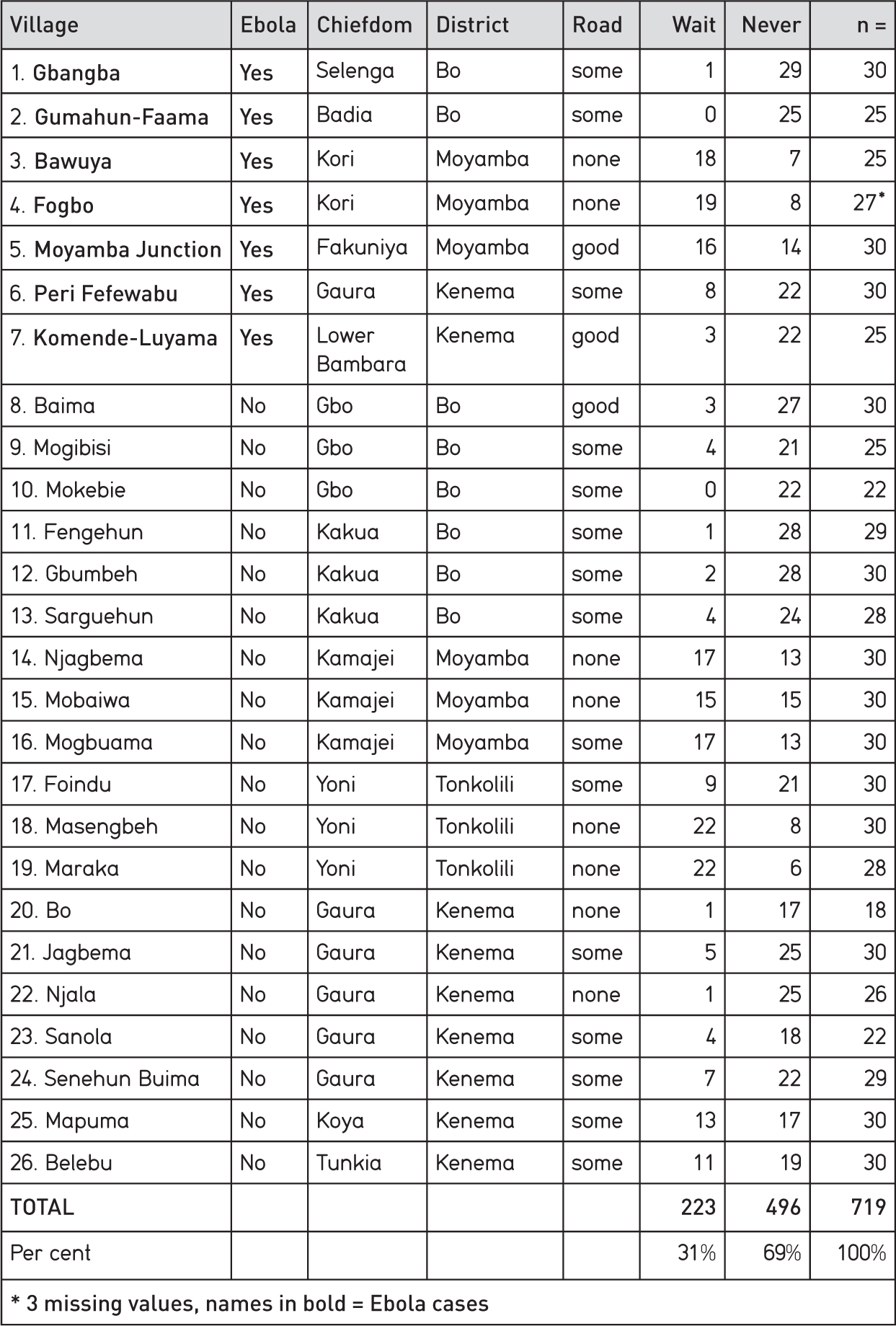
Seven villages with Ebola cases out of a sample of twenty-six over-represents the true community-level incidence of the disease, which is about one in forty villages, given a rough total of 16,000 village communities in Sierra Leone.5
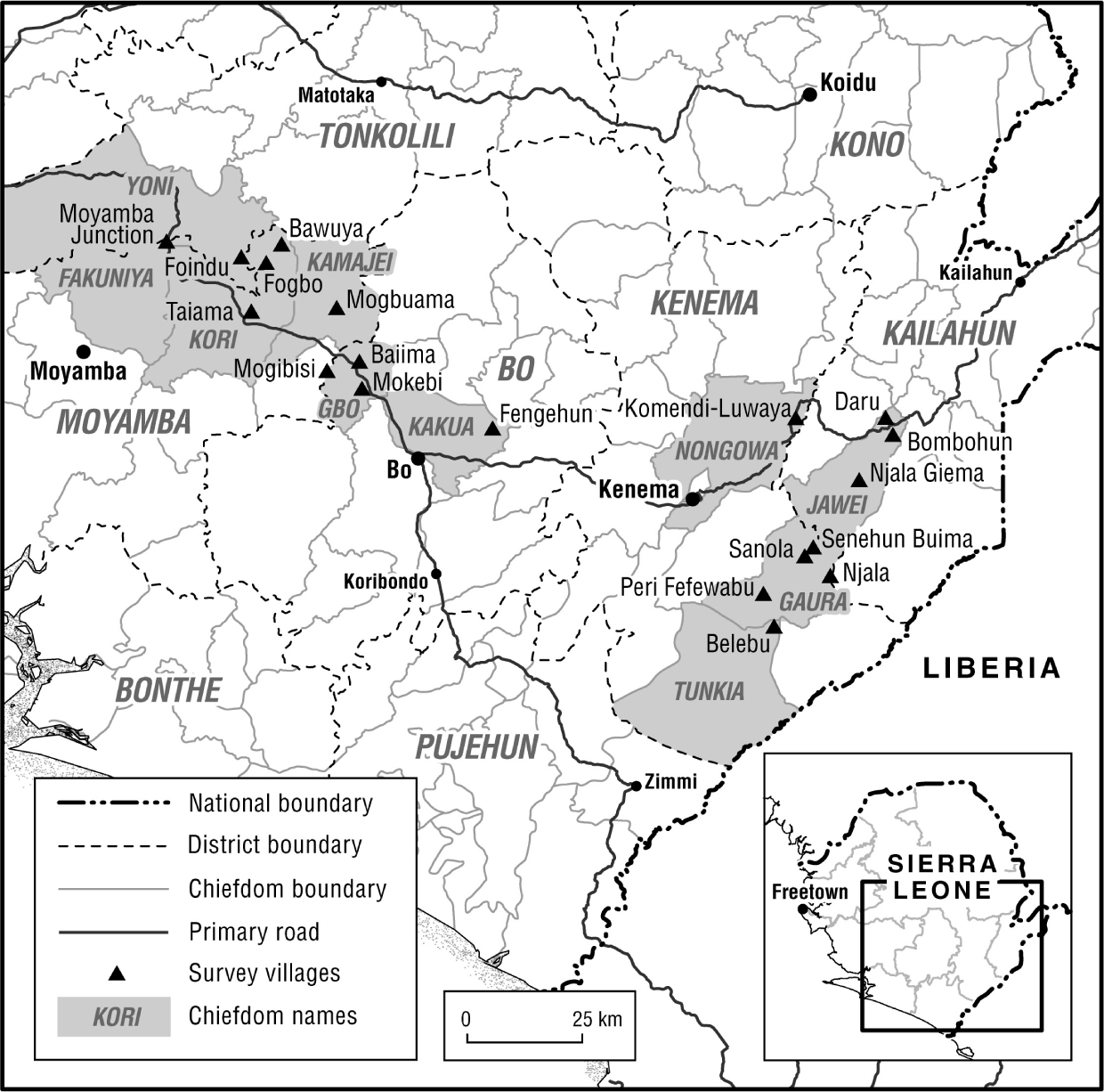
The research design selected a range of rural communities along a transect stretching from the Gola forest on the Liberian border, through Kenema District (Eastern Province), and Bo and Moyamba districts (Southern Province), to Tonkolili District in central-northern Sierra Leone. Most villages were Mende-speaking, but villages in Tonkolili District spoke Temne. Mende and Temne are the two main languages in rural Sierra Leone, in addition to Krio, widely spoken as a national lingua franca. There are some significant cultural differences between Mende and Temne communities, especially in regard to burial practices.
The material discussed below relates to three groups of villages. The first group comprised villages adjacent to the boundary between the northern and southern provinces, where there was an outbreak of Ebola in July/August centred on the village of Fogbo (Kori chiefdom), as briefly discussed in Chapter 2. This outbreak preceded the international response surge in the last three months of 2014. The second group comprises villages without Ebola cases in the general vicinity of the Fogbo outbreak, and served as a control. For one of these villages (Mogbuama) baseline data exist from 1983.6 The third group comprises villages in Kenema District in the east, adjacent to the Gola Rain Forest National Park, Sierra Leone’s last area of undisturbed tropical rainforest. Two of these villages experienced Ebola outbreaks in October/November 2014, and showed some evidence of the impact of the international response. Other (non-Ebola) villages were examined because of their closeness to the forest edge, thus illuminating potential problems of inaccessibility.
Figure 4.1 Villages in Tonkolili, Moyamba, Bo and Kenema districts surveyed as part of an Ebola impact study
Methods included a mix of quantitative and qualitative data-gathering techniques. A questionnaire was designed to elicit information from a random sample of around thirty adults per village (half of whom were female) on responses to sickness, including presumed causes of Ebola. Focus groups were organized to allow different groups of villagers (male elders, female elders, and youth - both male and female) to discuss a range of open-ended topics including causes of sickness and death, quarantine, normal ways of preparing corpses for burial, reactions to ‘safe burial’, ways of funding visits to health centres and other forms of medical care, and access to Ebola ambulances.7
When possible, the different focus groups were run simultaneously, to guarantee independence of viewpoint. Facilitators were trained to motivate discussions by moving from general to particular prompts. For instance, groups were asked to discuss common recent instances of sickness before any discussion of Ebola took place. Groups were encouraged to establish their own agenda of topics for discussion. Each group had a second facilitator to monitor side comments and body language.
Interventions were managed through a numbered card system. Each speaker traded in a card before making her or his point. This allowed coders to enter information on the types of person speaking, and the number of times they spoke, without compromising the anonymity of the speaker. All those answering questionnaires and participating in focus groups provided informed consent, and all personal names relating to victims, survivors and so forth were reduced to initials to preserve the anonymity of human subjects.
Descriptive analysis was undertaken based on tabulation of questionnaire responses, transcription and coding of focus group responses, comparison of responses for villages with and without Ebola, and assessment of intra-village variation, by gender and social seniority.
Village perspectives
What people thought caused Ebola
In the questionnaire survey two related questions were posed at different points in the interview:
Q. 1 What do you understand to be the causes of this sickness?
Q. 2 What is your own idea about how this disease spreads?
The first question was framed in general terms to avoid any imputation that the survey was checking up on the reception of Ebola messages. Nevertheless, respondents appear to have played safe, and said what they thought they were expected to say. But the second question differs, in that there is now a specific prompt. The interviewee is explicitly asked to say what he or she thinks.
This results in a clear shift in the balance of responses, and is here understood as evidence that people formed their own conclusions about causes, independent of messages received. Answers couched in terms of bushmeat significantly decline. Prominence is given to a new answer - that body contact is a key factor in spread of infection.8
Data relating to answers to the two questions were then examined for three Ebola village samples and four matched controls (see Table 4.2). Of the control villages, two were accessible by vehicle along farm access roads (Foindu and Mogbuama) and two (Mobai and Njagbema) were accessible only by footpath. About half of all males and 40 per cent of all females gave the answer that bushmeat was a major cause of Ebola infection in answer to Q. 1. This reduced to about 10 per cent when people were asked for their own understandings.9
Table 4.2 What people thought caused Ebola
Causes of Ebola as understood in general (Q. 1)
|
Males |
Females |
|
|
Bush meat a cause |
51 |
39 |
|
Bush meat not a cause |
52 |
63 |
Causes of Ebola as understood by respondent (Q. 2)
|
Males |
Females |
|
|
Bush meat a cause |
12 |
10 |
|
Bush meat not a cause |
91 |
92 |
Cross tabulation of answers to Q. 1 and 2
|
Q. 1 |
Q. 2 |
|
|
Bush meat a cause |
90 |
22 |
|
Bush meat not a cause |
115 |
183 |
There are no clear differences between communities with direct and indirect experience of Ebola. In both cases around 90 per cent of all villagers discounted bushmeat as a significant transmission pathway when describing their own beliefs about Ebola, and instead emphasize risk factors such as touching infected bodies. In other words, where public messaging concerning Ebola risks was wrong, as in the case of bushmeat, it was rejected in favour of risk factors with better empirical grounding in local experience.
The questionnaire also invited respondents to pose questions to the research team. These questions frequently implied scepticism about bushmeat as an infection pathway; for instance: ‘we have been eating bush meat for a very long time and have not experienced this disease, why only now?’.10 But despite this widespread scepticism many people, in fact, refrained from eating bushmeat, and saw this as something for which they should be compensated by the Ebola response; ‘[since] we have been asked not to eat bushmeat, then provide for us’ was one such blunt response.
It is also worth paying some attention to the ‘don’t know’ or ‘no answer’ responses (see Table 4.3). Fifteen women and twenty-one men provided answers of this sort, comprising 17.6 per cent of all answers, but 25.9 per cent of answers in communities with Ebola cases.11 It seems strange that lack of awareness of the causes of Ebola would be higher in villages with direct experience of the disease. These data may signal heightened distrust and a purposeful refusal to express a view.
Table 4.3 Negative (‘don’t know’ and ‘no answer’) and positive responses for villages with and without Ebola cases
|
Ebola village |
Non-Ebola village |
|
|
Negative answers |
22 |
14 |
|
Positive answers |
63 |
106 |
It is relevant to note that twelve negative (‘don’t know’ and ‘no answer’) answers came from people aged over sixty (one third of the total). Older people are more likely to be elders of the powerful sodalities, Poro and Sande. Sodality funeral practices have been implicated in Ebola transmission. The Fogbo outbreak was one such instance. Negative answers may suggest, therefore, the workings of sodality disciplines of secrecy rather than reflecting a poor state of factual knowledge concerning Ebola transmission pathways. This flags an issue, further addressed in Chapter 6, about the role of the sodalities in social mobilization against Ebola.
Access to treatment
The first requirement in an Ebola outbreak is to isolate confirmed Ebola cases in a special facility where palliative care can be safely administered. Hospitals unfamiliar with the necessary biosafety requirements spread the disease in the early stages of the epidemic, resulting in many deaths among medical staff, and dedicated Ebola Treatment Centres (ETCs) were established by agencies such as Médecins sans frontières to reduce nosocomial infection risks.
The disease moved across Sierra Leone from east to west, and then to the north-west. For a time, before the surge of international assistance in late 2014, ETCs were overwhelmed with demand, and sometimes turned patients away. Some patients were bussed long distance from newer infection areas in the west to longer-established facilities in the east, where case numbers were beginning to decline.
As a result of these long-distance movements of Ebola victims, families and patients became separated, and reporting of patient progress and outcomes to families was imperfect. Rumours spread about the alleged purpose of ETCs - to harvest body parts - and Ebola victims tried to avoid being taken to treatment centres. Some sought help from traditional healers (herbalists). The flight of these patients into the countryside reduced chances of survival, but increased the chances of new clusters of infection emerging.12
With the surge in international response, provision of beds began to catch up with need. New local holding and treatment centres (community care centres [CCCs]) were established at chiefdom and district level, and proved to be effective and acceptable.13 Communities were often positive about CCCs (despite the reservations of many responders) because they offered palliative care, free feeding (taken as evidence of goodwill) and after-care reintegration packages for survivors.
Even though staffed by volunteers with limited medical expertise, or even none at all, these centres did not become, as some had predicted, motors for the spread of the disease. There were few reports of staff infections, for example. The free care and feeding marked out the centres from previous healthcare provision. And because centres were local, families could keep an eye on loved ones, and follow outcomes. Most communities said they wanted such facilities repurposed rather than removed, once Ebola had gone. Clearly, they helped reduce fear, and increased local knowledge of the true nature of the disease.
The field study reported here was undertaken in December when many community care centres were still being built, especially in the north, where the epidemic was most actively spreading (see Figure 2.5 in Chapter 2). This was too early to assess their impact, but even so a key question could still be posed. Spread of Ebola would be reduced, and patient survival chances increased, if patients reported early (within the dry phase, generally lasting three days). So what, in general, influenced the speed with which villagers reported diseases to the health authorities?
In the questionnaire survey a random sample of fifteen male and fifteen female adults in twenty-six villages (see Table 4.1)14 was asked whether they ever hesitated to send a sick person to a health centre, and if so, by how many days they would delay for different classes of patient (children, adults and older people), and why. The three parallel focus groups in each of the villages were also asked to discuss access, finance and other obstacles to early reporting.
Of 719 persons interviewed 223 (just under a third) reported that they would wait for between one to three days to find out how the sickness progressed. In effect, they would sit out part or most of the dry phase of Ebola. With the onset of the wet phase it is too late to move a patient safely, except in a specialist ambulance, manned by a crew with protective clothing. Not all villages, of course, had roads, and hammocks would be the only alternative, at least as far as the roadhead. Hammock carriers have no protective clothing.
Data on waiting times were examined against a ranking of local road conditions. The aim was to ascertain whether prior experience of Ebola and poor road conditions influenced reporting times (see Table 4.4). No evidence was found that prior experience of Ebola reduced the chances of sending sick persons promptly for treatment, but poor road conditions did have a significant effect.
Did prior experience of Ebola make a difference in moving the sick? In villages without Ebola cases 33 per cent of persons said they would delay seeking help by one to three days or more. In villages with Ebola cases 37 per cent of persons said they would delay seeking help by three days or more (Table 4.4).
Table 4.4 Whether experience of Ebola cases and lack of road access reduce chances of patients moving to medical care
|
Move |
No move |
|
|
Ebola |
105 (110.27) [0.25] |
62 (56.73) [0.49] |
|
No Ebola |
276 (270.73) [0.1] |
134 (139.27) [0.2] |
|
Move |
No move |
|
|
No road access |
99 (134.99) [9.6] |
115 (79.01) [16.39] |
|
Some road access |
282 (246.01) [5.27] |
108 (143.99) [9] |
Did road access make a difference to delay in moving the sick? In eight villages with no road access 52 per cent of persons interviewed would wait up to three days or more before seeking medical help. In eighteen villages with (some) road access only 22 per cent of persons would delay seeking help by three days or more (Table 4.4).
Note that the three Ebola-affected villages in the Fogbo outbreak (Fogbo, Bawuya and Moyamba Junction) all had a high likelihood of persons not moving immediately for medical assistance. However, the same was also true of three control villages without Ebola in neighbouring Kamajei chiefdom (see Table 4.1). Note also that Moyamba Junction has very good road communications; high waiting times cannot be a reflection of poor road conditions in this specific case.
How were delays explained?
When asked directly about their personal experience (‘had they ever been too sick to seek help outside the village?’) nine people in Bawuya, a small off-road village infected with Ebola from the Fogbo outbreak, answered ‘yes’. Lack of money and quarantine restrictions were the major reasons given.
This set of answers included all three Ebola survivors in Bawuya. In earlier answers, two of these survivors described being treated in an Ebola Treatment Centre (ETC). The final stage of both these journeys was in an Ebola ambulance. Thus these answers might be taken to imply that reaching an ETC might not have been the original intention, but a decision taken for them by the authorities.
Interviewees were then asked, in the case that a member of their household had a fever, which of three statements was more likely to be true: take them to a hospital immediately, wait for some time to see whether they get better, or never take them to a hospital. As noted above, early reporting of Ebola cases is crucial to improved chances of survival. Only seven respondents said they would act immediately. Seventeen would wait.15
People were also asked how long they would wait if the case involved a child, an adult or an old person. Respondents provided estimates in terms of days or fractions of days they would spend waiting. For a child the waiting time ranged from one hour to seven days (average = 1.2 days). For an adult the time was longer, ranging from one to eight days (average for adults = 2.1, average for older people = 2.0).
Reasons were given to explain these differences. Children, it was frequently suggested, were weaker than adults, and could die more quickly. Views on older people were split. Some thought that they should be taken for treatment as soon as possible, but one respondent reckoned on a delay by a day for a child, three days for an adult, and a week for an older person, bluntly commenting that ‘old people are always sick’. Another person thought there should be no difference between children, adults and the elderly (‘all are humans’). Even so, this respondent would wait a full day before seeking help.
In Fogbo, the decision to wait before seeking medical help was reported by seventeen interviewees. Average waiting times before seeking medical help were similar for both children and adults (children 1.1 and adults 1.0 days), but somewhat longer for older people (2.1 days).
Lack of money was offered as a reason to delay in two cases. Once again one person openly voiced the idea that older people are ‘always sick’, and that it was impossible to respond to every case. The somewhat longer waiting times in Bawuya, compared to Fogbo, probably reflect the fact that Bawuya is three hours’ walking distance from medical treatment in Taiama, whereas Fogbo has its own medical post.
For comparison, it is interesting to look at focus group results for Bo-Gaura, an off-road forest-edge village on the margins of the Gola forest in the east of country. The account was pieced together from comments made by members of all three focus groups, and provides a graphic picture of what medical evacuation, for Ebola, or any other disease, would entail in these remote and isolated conditions:
[The] road is not motorable and people use hammocks to carry people to health facilities at a distance. Travelling is mostly at night, [and there are] lots of hills in this community.
Most of the bridges are made of wood, [are] not strong, and you get hungry when trying [hard] with the hammock.
Money is needed, for support to young men, [this includes] provision of torchlight for night travel, and rain gear for travelling during the raining season.
[If such movement is needed] a family meeting will be summoned and every one [is] asked to contribute money to pay for transportation and treatment fee, and to ‘beg’ [i.e. motivate the] youths to transport [a] sick person in [the] hammock to the nearest health centre.
Family members are taxed, married children are asked to pay some amount, and youths are begged to carry the sick if the road is not accessible by vehicle or bike.16
Off-road villages maintain hammocks for emergencies of necessity, and young men are skilled in transporting sick people in them. Hammock travel is a specific technique of the body with its own hazards.
[The] hammock swings, [so there is risk that the] carrier will contract sickness from [an Ebola] patient.
Bo-Gaura had had no Ebola cases, so this remark is evidence that villagers were able ‘to think like epidemiologists’, in inferring potential infection risks for a disease not yet experienced directly.
If treatment is needed in a health centre outside the village cost issues become major constraints. Money is needed both for the hammock ride, or to charter a motorbike taxi, and then to pay for medication, treatment and feeding. A night-time or rainy-season ride is an especially expensive proposition, since the evacuation team will also need torches and/or rain gear. It is not hard to understand why villagers with few or no savings hesitate to rush for medical treatment.
[My] son was treated at home not in hospital because money was not available. He was given local herbs to drink.17
[To move a sick person] we will use motorbikes and it will cost Le 15,000 [about $3.00, or about a day’s wages for a farm labourer] from Peri to Joru health centre [a distance of about five kilometres]. [The decision to move a person will be taken by] the chief and family members. For a stranger, the hotakei [lit. stranger father, landlord] will decide on carrying the sick person. [If there is no money] the family member, town’s people and the person accommodating the stranger will contribute to pay the money. If the money contributed is not enough, we will pledge the person’s plantation or property to pay the money.18
Sick people are taken to Fogbo or Taiama by hammock or okada [motorcycle taxi], where hospitals are available.19
Family members will inform the chief, who in turn will inform the youth leader [Ndakpo mahei, literally ‘chief of the age mates’]. The hammock will be used and youths given a small token as motivation.
In Mogbisi, Gbo chiefdom, Bo District, female elders offered the following description of how care for the sick is organized (see tabulated responses in Table 4.5). A husband, wife or older child will take charge of the nursing. For a woman the carers will be members of her own lineage (ndehun). For wives born outside the village (see below) this implies either moving the patient back home, or that a person from the home village will move to the sick woman’s marital location to offer care. In cases of Ebola such mobility could be a factor in inter-village spread of the disease.
Table 4.5 Comments on care, by female elders of Mogbisi, Gbo chiefdom
|
Who cares for seriously sick persons? |
‘If a man, he will be cared for by his wife and eldest son, if a woman by the daughter.’ |
|
Who cares for an adult woman when sick? |
‘The relatives from the family of the sick person. Sometimes her peer group.’ |
|
If a man or woman has no husband or wife who cares for him or her? |
‘The relatives of either side, or [if a] stranger, the host.’ |
|
If the sickness cannot be cared for in the village, what arrangement will send the sick person to a hospital or health centre in [an]other location? |
‘The chief and the family will gather the community to loan money from within the community or club (osusu) for medication.’ |
|
If there is no money to carry the sick [person] what will happen? |
‘The family will loan or sell their land and plantation.’ |
Serious sickness generally involves arranging a loan, pledging of tree crops or selling of land (see comments of the youth focus group in Peri Fefewabu above). The link between recurrent sickness and endemic impoverishment is a long-term feature of agrarian poverty in rural Sierra Leone.20
Calling for help
The National Ebola Response Commission established a telephone ‘hotline’ (‘117’) to process requests for burial and evacuation of sick persons by ambulance. After initial problems the helpline scaled up, and appears to have worked quite well in urban and peri-urban areas of Freetown and the main provincial towns, from which (in the end) a large proportion of Ebola cases came.
Western Area - greater Freetown - alone accounted for about 40 per cent of all confirmed Ebola cases. However, the helpline suffered from the incomplete national cell phone coverage (only about 70 per cent of the country) and the difficulties routinely experienced in rural areas of keeping mobile phones charged. Charging phones is a thriving cottage industry for owners of small generators in many larger villages, but is not easily afforded by all. Many phones need to be charged once an emergency arises, adding to response times.
Figure 4.2 shows these blank spots. Coverage gaps are especially significant in Koinadugu District. Owing to its isolation this district had few Ebola cases overall, but there was an important outbreak in Neini chiefdom, an alluvial gold mining area at the centre of the district, with no cell phone coverage.
Figure 4.2 National cell phone coverage at October 2014
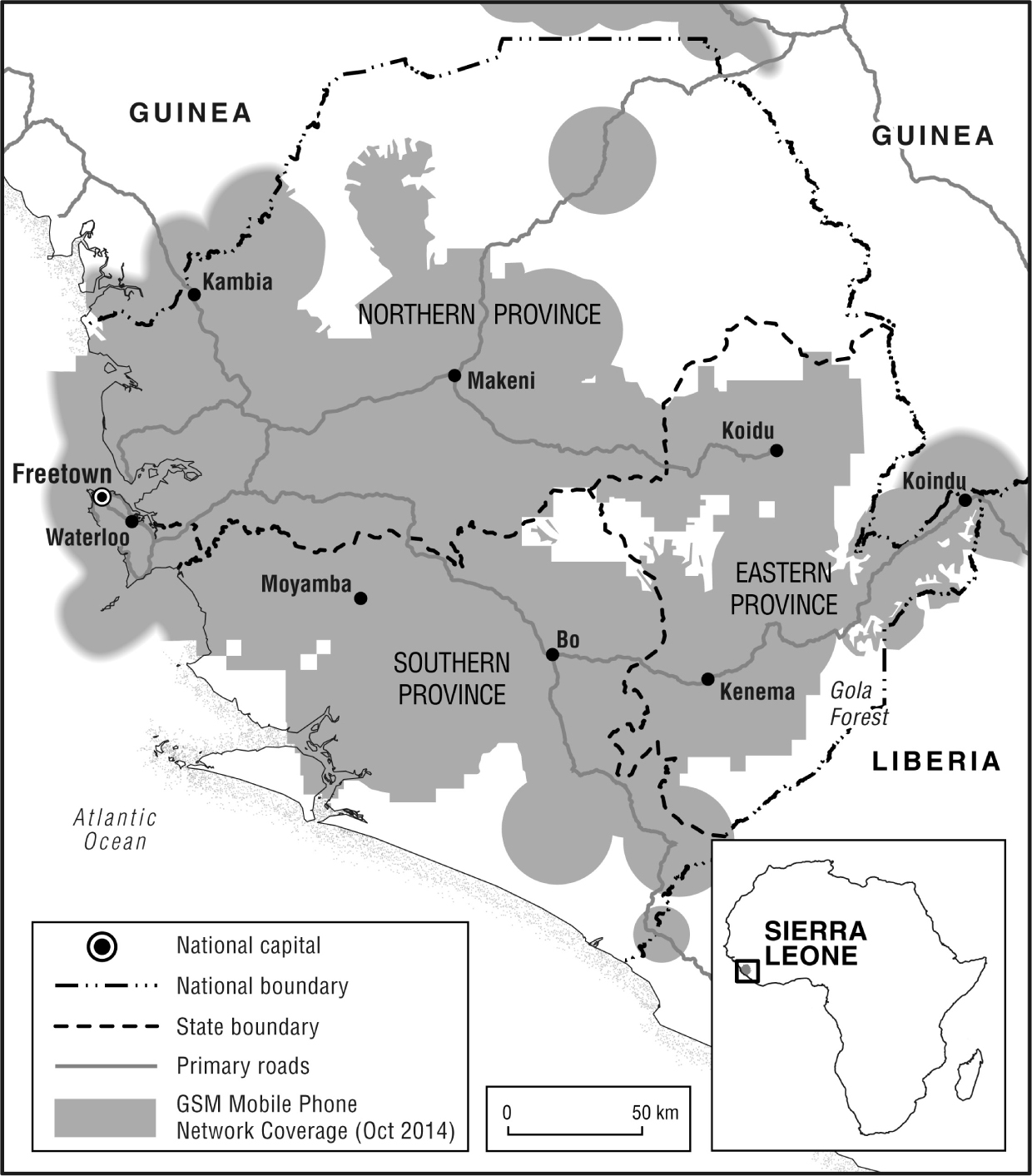
A communications gap around the margins of the Gola forest should also be noted. This is hilly terrain, and even when coverage is indicated, villagers often need to seek higher ground to get a signal. Peri Fefewabu - an outbreak village - is one such place. Lack of phone coverage in an area at risk of zoonotic spillover might be a serious issue if outbreaks were to recur.
Movement of the body at death
The likelihood of bodies travelling home in pre-Ebola times has been indicated in the fieldwork vignette above. Such movements were especially likely for women, for reasons already indicated, or for the bodies of urban residents who had maintained a strong identity with their rural home (typically, first-generation migrants).
Many males wanted their bodies to be repatriated to be close to the focus of family life. A publicly known place of burial is especially important where the family has rights to land or chieftaincy. In recent times, grave sites have taken on an increased importance with the rising value of rural land for agricultural investment. In a patrilineal community, repatriated male bodies help guard the land rights of descendants of deceased persons.
In the case of a wife, the husband has to give an account to the family of the cause and circumstances of death. He will fight hard to get the body of his wife home, not least to dispel any suspicion among her family that the woman died of mistreatment or neglect.
A need to move the body is not only confined to urban migrants. Rural-rural movement is also likely at death, especially where the deceased person had the socio-legal status of a stranger (hota, in Mende).
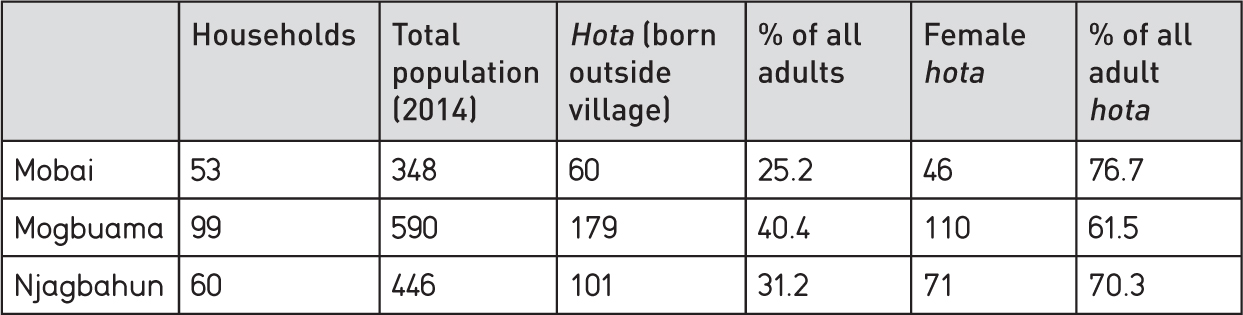
Strangers are recognized in customary law as persons living outside their chiefdom (or sometimes village) of birth. A survey of three villages in Kamajei chiefdom in early 2014 offers evidence of the typical proportions of village populations classed as strangers (from 25 to 40 per cent).
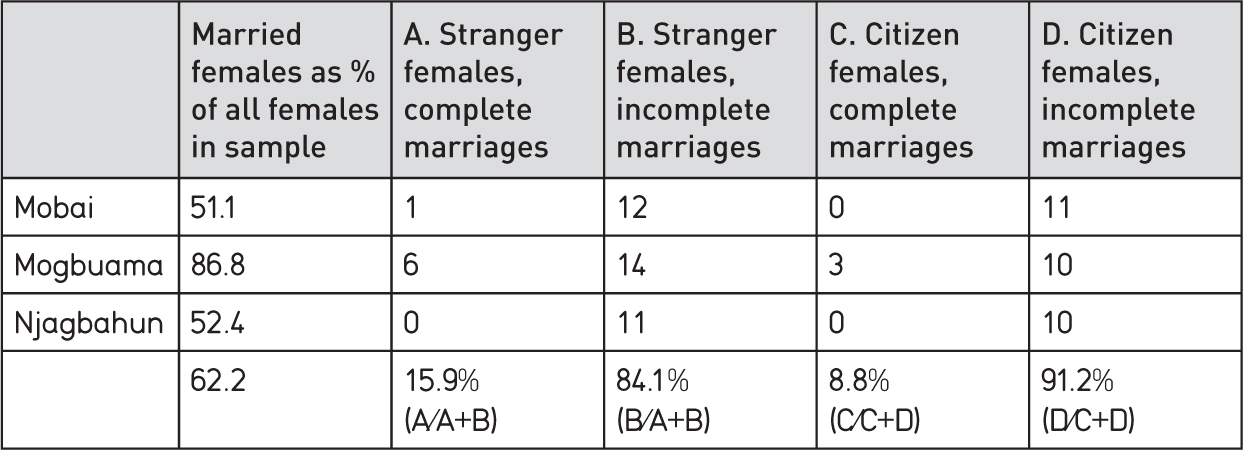
About one third of all residents of the three villages recorded in Table 4.6 were classed as strangers. One quarter to one third of this stranger group was male. Thus the bodies of about 8-10 per cent (0.33 x 0.25, or x 0.33) of male village residents are liable to be taken home after death. But it will also be noted from Table 4.6 that about two-thirds to three-quarters of all strangers are women. This is because many rural women (typically 40-50 per cent) marry outside their home villages. Rural marriage in Sierra Leone is predominantly virilocal (i.e. the woman moves to her husband’s home village). Whether the body of the wife is then buried in the husband’s village or the woman’s home depends (as noted) on the status of the marriage payment.
Many village marriage payments remain incomplete for years. Farming life is hazardous, and farmers are in the grip of poverty. Promises to the family of a farmer’s wife may have to be deferred owing to misfortune and lack of resources. The wife’s body will be reclaimed by her family unless debts are quickly settled post-mortem.
Table 4.6
a) Stranger origins in 3 villages in Kamajei chiefdom, 2014
b) Rates of marriage completion, 3 villages in Kamajei, 2014
Any such post-mortem movement was forbidden by emergency regulations covering the Ebola epidemic in Sierra Leone, and all burials, irrespective of cause, were (supposedly) carried out as rapidly as possible by ‘safe burial’ teams. But this represented a large legacy of ‘incorrect’ burials. How this legacy will be dealt with in the post-Ebola era remains to be seen. There might be some pressure for reburial. A basic requirement under Ebola regulations for ‘safe burials’ is for these to be properly documented. Failure to address the reasons for ‘home’ burial might have lasting adverse consequences for rural land tenure arrangements and social cohesion.