An Introduction to Applied Cognitive Psychology - David Groome, Anthony Esgate, Michael W. Eysenck (2016)
Chapter 10. The effects of drugs on cognition
Moira Maguire
10.1 INTRODUCTION
Drugs are substances, natural or synthetic, that produce physiological changes when taken into the body. In the case of drugs used in the treatment of disease, these changes act to treat disease or to manage pain or other symptoms. We can distinguish between these medications and drugs that are consumed for their psychoactive effects, i.e. the effects they have on mood, cognition and experience. Psychopharmacology is the study of the effects of drugs on the nervous system and behaviour.
Psychoactive drugs alter activity at nervous system synapses. A synapse is the place where messages pass from one neuron to another. Chemicals known as neurotransmitters pass the messages from neuron to neuron. Drugs can impact on the activity of neurotransmitters, either directly or indirectly. An agonist increases the action of a given neurotransmitter whereas an antagonist decreases or blocks it.
Many of these drugs are potentially addictive and/or have a high potential for abuse. Most addictive drugs (like other potentially addictive phenomena such as gambling) stimulate the release of the neurotransmitter dopamine (DA) in the nucleus accumbens (Blum et al., 2012). The nucleus accumbens forms part of the mesolimbic dopaminergic reward system in the brain (see Figure 10.1). This system regulates responses to rewards and is important in motivation. People differ in their vulnerability to drug abuse, with biological factors, personal characteristics and wider social factors all playing their part.
This chapter is concerned with the effects of both the legal, ‘social’ drugs and illegal drugs on cognitive performance. These effects are of interest to cognitive psychologists for a number of reasons. Drugs can be used as research tools to manipulate the activity of particular neurotransmitters and examine the effects on cognition. In this way, drugs can tell us much about the biological basis of cognition. Second, since the majority of people use drugs such as caffeine on a daily basis, it is important for students of applied cognition to understand if, how and when these substances affect performance. This research can also help us to understand why people use substances such as nicotine and caffeine.
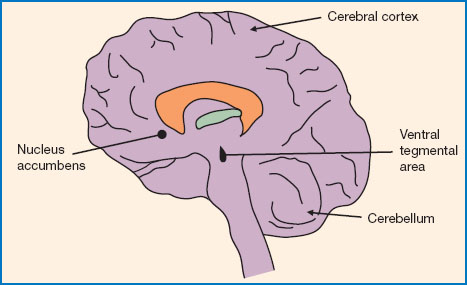
Figure 10.1 The location of the nucleus accumbens in the human brain. Both the nucleus accumbens and the ventral tegmental area (VTA) form part of the reward system. Dopaminergic neurons in the VTA project to the nucleus accumbens and other areas of the forebrain. This pathway is part of the medial forebrain bundle (MFB) and is a critical part of the brain reward system.
THE SOCIAL DRUGS
The term ‘social drugs’ refers to caffeine, alcohol and nicotine: substances that are legal and used routinely by people in everyday life. While alcohol and nicotine (tobacco) are legal, their use is regulated in most jurisdictions as they are associated with health and social costs.
People drink coffee and alcohol and smoke tobacco for many different reasons. These behaviours have important social dimensions: many of us relax and meet friends over a coffee or a drink. Smoking and other nicotine use (e.g. chewing tobacco) is always harmful to health, and smoking is the biggest single cause of preventable deaths in Europe and the US. Most smokers report that they want to stop smoking, but this can be very difficult. Smoking has important social dimensions and is a complex behaviour that is used by smokers in different ways and to fulfil different needs (Graham, 1994; Collins et al., 2002). However, there is some evidence to suggest that behaviours such as drinking coffee and smoking may be partly maintained because of the effects they have on cognitive performance.
ILLICIT DRUGS
Illicit drugs include cannabis, heroin, cocaine, amphetamines and ecstasy, and all have a high potential for abuse. Drug abuse is a major social problem in most Western countries and is strongly associated with crime. A small minority of people use these drugs, and recreational drug use is higher among young people than other age groups and higher among men than women. The 2013/14 Crime Survey for England and Wales found the prevalence of the previous year’s illegal drug use to be 8.8 per cent. This is considerably lower than the 12 per cent typically reported in the late 1990s (Burton et al., 2014). Cannabis is the most commonly used drug, followed by cocaine and ecstasy, and it is these that will be considered in this chapter.
10.2 CAFFEINE
Caffeine is probably the most widely used psychoactive substance in the world. It is naturally produced by many plants, including the coffee and cocoa plants. Sheppard (2013) suggests that caffeine may be used by plants to ensure pollination by bees through ‘strengthening honeybee neuronal connections between a general-specific floral scent and reward pathways associated with nectar sweetness’ (p. 1202).
Caffeine is an alkaloid that belongs to a class of chemicals known as the methylxanthines. It acts to increase nervous system arousal (Barry et al., 2008) and is an antagonist for adenosine (Cauli and Morelli, 2005). Adenosine is important in the sleep/wake cycle - it helps to tell us that we’re tired by inhibiting neural activity. So, when caffeine binds to adensoine receptors, instead of the inhibitory effects of adenosine, we get the stimulating effects of caffeine. It increases arousal in both the central and sympathetic nervous systems.
Caffeine is consumed in many different substances, particularly coffee, tea, caffeinated soft drinks such as colas, chocolate and headache and cold remedies. It is absorbed quickly and reaches peak levels in blood plasma after approximately 30 minutes when taken orally (Barry et al., 2008). Table 10.1 shows the approximate caffeine content of a range of common dietary sources.
Heavy users of caffeine sometimes report withdrawal symptoms after ceasing use. The most common of these are fatigue and headaches, but some people also experience anxiety, nausea, weakness and depression (Griffiths and Woodson, 1988). Streufert et al. (1995) examined caffeine withdrawal in twenty-five managers who were heavy caffeine consumers (mean daily intake was 575 mg). After 36 hours’ abstinence their performance in managerial simulations had significantly declined. This, and other evidence, suggests that people can become dependent on caffeine and suffer withdrawal symptoms.
Table 10.1 The most common dietary sources of caffeine. There is considerable variation in the caffeine content of each source. Some of the very large coffees offered by coffee-chains can contain well over 300 mg per serving! The recommended daily allowance is 400 mg, dropping to 200 mg during pregnancy
|
Source |
Amount of caffeine in milligrams (mg) |
|
Espresso coffee |
50-75 mg |
|
Percolated coffee (mug) |
100-200 mg |
|
Instant coffee (mug) |
30-170 mg, typically 60-100 mg |
|
Tea (mug) |
20-70 mg, typically 30-40 mg |
|
Cola drinks (per can) |
23-47 mg, depending on brand and type |
|
Energy drinks (approx. 250 ml) |
70-100 mg, depending on brand |
|
Dark chocolate (50 g bar) |
10-35 mg |
|
Milk chocolate (50g bar) |
6-12 mg |
|
Cold and flu remedies |
25-30 mg per tablet typical for those that do contain caffeine |

Figure 10.2 Caffeine is probably the most widely used psychoactive substance in the world. It is generally consumed in drinks such as coffee (above), tea or soft drinks, but is also present in chocolate, medications and increasingly, in cosmetics.
Source: FreeImages.com/ Andreas Just.
METHODOLOGICAL ISSUES IN RESEARCH ON CAFFEINE
As you will see below, the evidence regarding effects of caffeine on cognition is quite mixed. This may be, at least in part, due to difficulties comparing studies. The research on caffeine, and the other social drugs, takes a number of approaches. Some studies focus on caffeine-deprivation, others are concerned with the effects of particular doses of caffeine or dose-dependency relationships, while some researchers use caffeine as a tool to manipulate arousal. This means that studies are often concerned with very different things. Furthermore, there is a huge range in the dosages used - from approximately 30 to 600 mg. Some use a single dose, such as 100 mg, while others provide doses relative to body size (mg/kg). There is also considerable variation in design and control measures, such as washout periods and time of day. To further complicate matters, the range of dependent variables that has been studied is enormous, making comparisons even more difficult (Koelega, 1998). These problems can also be seen in the study of the other social drugs. There is a need for greater standardisation for procedures and tasks to facilitate study comparisons and achieve a greater understanding of the effects of caffeine on human cognition, performance and mood.
Table 10.2 Evidence regarding the effects of caffeine on cognition and performance is inconsistent and methodological differences can make it difficult to compare studies. The key inconsistencies are summarised below
|
Studies of caffeine and cognitive performance are difficult to compare as they vary in terms of: |
|
✵ Research question and focus ✵ Dosage ✵ Control measures, such as washout periods and time of day ✵ Participants - age, gender, smoking status etc. ✵ Dependent variables |
THE EFFECTS OF CAFFEINE ON COGNITIVE PERFORMANCE
Caffeine is generally recognised as enhancing cognition. It has been shown to facilitate performance on vigilance tasks, simple and choice reaction times, letter cancellation, tapping, critical flicker fusion thresholds (CFFT) and some aspects of motor performance (see van der Stelt and Snel, 1998 for review), although there is debate about whether these are genuine effects (James, 2014). The most reliable benefits of caffeine have been found on alertness and processing speed.
ALERTNESS, ATTENTION AND REACTION TIME
The beneficial effects of caffeine on alertness are well documented and a decrease in alertness is an often-reported symptom of caffeine withdrawal. Evidence is mixed regarding attention. Hogervorst et al. (2008) found a 100 g dose of caffeine to improve performance on the Stroop effect, but other research has reported no effects and there is inconsistent evidence regarding divided attention (van der Stelt and Snel, 1998).
Many studies have shown caffeine to improve both simple and choice reaction time. Kerr et al. (1991) found that choice reaction time was facilitated by caffeine and that this was largely due to effects on the motor component of the response. Lieberman et al. (1987) reported positive effects of low and moderate doses on vigilance and choice reaction time. Beneficial effects of caffeine on rapid visual information processing, response speed and concentration have also been reported by Hogervorst et al. (2008).
Where improvement is found, it is generally in the form of a decrease in time taken to respond (faster reaction time), rather than an increase in accuracy. It seems that caffeine can improve the perceptual input and motor output aspects of these tasks rather than the cognitive, or response choice aspects (van der Stelt and Snel, 1998). Nonetheless, the picture is far from clear, as other studies have failed to show any effects. Rogers et al. (2013) investigated the effects of of 100 mg and 150 mg of caffeine on simple and choice reaction time, recognition memory, altertness, sleepiness and anxiety. They took habitual caffeine consumption into account. They found that overnight abstinence had negative effects on alertness and reaction time. Caffeine reversed these negative effects for medium to high consumers but there was no net gain (see below for discussion of genuine effects vs alleviation of withdrawal). While caffeine reduced sleepiness in those who had an intake <40 mg per day, alertness didn’t improve as it was offset by an increase in anxiety. The authors suggest that tolerance may develop, so that caffeine fails to cognitively enhance heavy users.
There is increasing interest in the effects of caffeine on reaction time in skilled performance, particularly in sport. In general, this evidence indicates beneficial effects of caffeine on speed, power, attention, reaction time and agility (see Santos et al., 2014). For example, Hogervorst et al. (2008) found caffeine, administered via a nutrition bar, to significantly improve both physical endurance and cognitive performance in athletes. These effects may be complex: Santos et al. (2014) found a 5 mg/kg dose of caffeine improved reaction time in a simulated taekwondo contest, but only in the early stages. Caffeine also seemed to delay fatigue. The authors concluded that caffeine can be used to increase intensity of taekwondo training and improve performance.
MEMORY AND LEARNING
The evidence is very inconsistent regarding memory and learning. A number of studies have reported beneficial effects of caffeine on recall (e.g. Arnold et al., 1987), while others found either no effects or detrimental effects (e.g. Loke, 1993). Warburton (1995) reported beneficial effects of low doses of caffeine on problem solving and delayed recall, but not on immediate recall or working memory. Using a 40 mg dose (about the amount in a cup of tea), Smith et al. (1999) reported no effect of caffeine on free recall, but it did increase speed of response in a delayed recognition memory task. Kelemen and Creeley (2001) found that a 4 mg/kg dose of caffeine facilitated free recall, but not cued recall or recognition memory. Miller and Miller (1996) reported that 3 mg/kg and 5 mg/kg doses of caffeine improved learning, but Loke et al. (1985) had found no effect of similar doses.
Klaassen et al. (2013) examined the effect of a dietary dose (100 mg) of caffeine on working memory in middle-aged men. The participants all used caffeine habitually and were tested at the end of their working day. They were allowed to consume caffeine as normal throughout the day to ensure that they were not in a state of withdrawal. Working memory was assessed using a version of the Sternberg letter task. Participants were asked to memorise a string of letters displayed for 4 seconds on a screen. Working memory load was manipulated by varying the length of these strings from three to six letters, which was followed by fixation on a cross in the centre of the screen for 3-6 seconds. Finally a probe letter was presented and participants were asked to identify whether it had been part of the original display. An interesting feature of this study was the use of functional magnetic resonance imaging (fMRI) to explore the effects of caffeine on the brain and link these to performance, and the fMRI results suggested that caffeine directly affects the fronto-parietal working memory system but also has indirect effects via arousal. The effects of caffeine were related to the difficulty of the task: at high levels of working memory load, caffeine seemed to impair performance. So, while a good deal of evidence suggests that acute doses of caffeine can improve learning and memory, other evidence suggests that caffeine either has no effects or tends to impair memory, and this equivocal picture is probably linked to the methodological issues discussed earlier.
While much of the experimental work is concerned with acute doses of caffeine, there is increasing interest in the cognitive effects of habitual caffeine use. Hameleers et al. (2000) found that caffeine intake was positively associated with performance in a delayed recall task and faster reaction time in a sample of 1875 adults. There was an inverted- U relationship between caffeine consumption and reading speed: increased speed was associated with higher caffeine intake up to five units of caffeine and thereafter the relationship was negative. There was no relation ship found between caffeine consumption and short-term memory, planning, information processing or attention. More recently, Kyle et al. (2010) explored the association between self-reported caffeine intake and cognitive performance in a sample of 325 Scottish older adults. They found that higher caffeine intake was associated with poorer performance on the Digit Symbol Substitution Task (DSST), but that this was confounded by socio-economic status. When this was controlled for, the association disappeared, leaving no relationship between caffeine intake and performance.
Of particular interest currently is the relationship between habitual caffeine intake and risk of dementia. Dementia is a condition characterised by significant memory impairment, and there are many causes, with Alzheimer’s disease (AD) being one of the best known but certainly not the only one. Dementia is by no means an inevitable part of ageing, but the prevalence does increase with age. Unsurprisingly, there is a considerable amount of epidemiological research that focuses on the associations between exercise, smoking patterns, diet and dementia. Again, the evidence regarding caffeine is mixed. In a sample of over 7,000 older adults, Ritchie et al. (2007) found evidence that caffeine had a protective effect against cognitive decline, but only for women who did not have dementia. There was no effect of caffeine on the risk of dementia over 4 years. In a 2010 systematic review and meta-analysis, however, Santos and colleagues (2010) found that the evidence did suggest that caffeine had some degree of protective effect. Again, it is very difficult to draw any firm conclusions as the studies differ so widely in their methodologies. Some are concerned with AD, others with dementia more generally and still others with cognitive decline. Caffeine consumption is measured in different ways and few studies take account of the duration of exposure to caffeine. Caffeine intake is also confounded with other variables that affect dementia risk, such as hypertension and smoking. Santos et al. conclude:
Setting consensual criteria for the definition of outcome as well as creating defined categories and types of exposure might be useful in conducting meta-analyses, and increase statistical power for the detection of an association between caffeine and cognitive impairment or dementia. (Santos et al., 2010, p. 230)
CAFFEINE AND LOW AROUSAL
Undoubtedly caffeine has beneficial effects on performance in low-arousal conditions. Attention often decreases in the early afternoon and this is called the ‘post-lunch dip’. Smith et al. (1990) found that caffeine removed this ‘dip’ in a sustained attention task. Caffeine has also been shown to sustain performance during prolonged work and to enable those with colds to compensate for impaired performance on a reaction-time task (Smith, 1998).
Sleep loss reliably produces decrements in performance, but caffeine has been shown to improve alertness during night-work when taken at the beginning of a shift. Bonnet and Arnaud (1994) examined the effects of both a 4-hour nap and caffeine on the performance of sleep-deprived participants (illustrated in Figure 10.3). They assigned male volunteers to either a caffeine or a placebo group. Participants in both groups were given tablets that contained either caffeine (caffeine group) or no active ingredient (placebo group). All participants had baseline data taken in the morning, after a normal night’s sleep. Later that day they took a 4-hour nap (4pm to 8pm). This was followed by 27 hours of alternating performance and mood tests, breaks and observations. Those in the caffeine group maintained roughly baseline levels of performance and alertness across the night, whereas those in the placebo group showed significant deterioration in their performance. These findings demonstrated that the combination of a prophylactic nap and caffeine was significantly more beneficial in terms of maintaining performance and alertness than a nap alone.
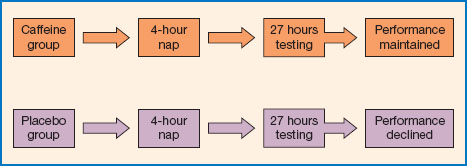
Figure 10.3 Bonnet and Arnaud (1994) found that caffeine could enable sleep-deprived participants to maintain baseline levels of performance.
As noted earlier, there is some controversy about whether the effects of caffeine are true effects per se or whether caffeine simply increases arousal or performance to a more optimum level. James (1994, 2014) has argued that positive effects of caffeine in laboratory experiments may be due to an alleviation of caffeine withdrawal rather than genuine benefits. Given the need to ensure that doses are similar for all participants, washout periods are used. Participants are asked to abstain from all caffeine, and usually alcohol and tobacco as well, for a given period of time before the experiment begins. However, the longer the washout period, the more likely it is that the individual is experiencing some degree of caffeine withdrawal. As James (2014) points out, many researchers take advantage of the natural overnight washout and ask participants to refrain from their morning caffeine, but this acts to increase the likelihood of withdrawal. So where we see improvements in a caffeine condition relative to a control, this may well reflect alleviation of withdrawal. Long-term withdrawal (over a period of days or weeks) is increasingly being used as an alternative design. James (2014) argues that work using these designs typically finds no effects of caffeine, supporting his argument that the effects are not genuine. Using caffeine-naïve participants is another option. These are people who use little or no caffeine, so cannot be in a state of withdrawal. Of course, these people are unrepresentative and are likely to differ in terms of their physiological response to caffeine, making findings ungeneralisable. There is also the possibility that the benefits people report from drinking coffee and tea have non-pharmacological components, for example the act of drinking a cup of coffee itself may be beneficial. However, while this may be important in everyday life, it is unlikely to explain the effects reported in experimental studies, as positive effects have also been found when caffeine is administered in tablet form. Moreover, Smith et al. (1999) compared the effects of a single 40 mg dose of caffeine administered in different forms: tea, coffee, cola, tap water and sparkling water. They found that the effects of caffeine were independent of the type of drink in which it was administered and concluded that ‘The overall conclusion is that caffeine is the major factor related to mood and performance changes induced by caffeinated beverages’ (p. 481).
Whether or not caffeine genuinely improves cognitive function or reverses deficits caused by withdrawal, it is clear that for the majority of the caffeine-using population, it can be used to enhance aspects of cognitive function and is especially effective when we are not at our best.
CONCLUSIONS
While it is clear that caffeine reliably increases alertness and aspects of psychomotor speed, the evidence is inconsistent regarding other areas of cognitive performance. A good deal of this inconsistency seems to be due to the wide range of methodologies used, which renders comparisons difficult. However, on the basis of the evidence we can conclude that caffeine does affect human cognition and performance, generally in a positive way, and these benefits may underpin the use of coffee and tea in everyday life. Specifically we can conclude:
✵ Caffeine tends to reduce performance decrements under sub-optimal conditions (e.g. fatigue, hangover, colds and flu).
✵ Caffeine facilitates alertness.
✵ Cognitive tasks involving ‘speed’ rather than ‘power’ may be particularly sensitive to caffeine.
✵ Caffeine reliably improves vigilance performance and decreases hand steadiness.
✵ Beneficial effects of caffeine can be observed even at low doses (<40 mg).
So, caffeine may achieve its effects through indirect and direct mechanisms. Indirectly caffeine may affect a general arousal factor, particularly under sub-optimal conditions. Caffeine may also affect a specific speed or efficiency factor and this would make some aspects of cognitive performance more sensitive to caffeine than others.
10.3 ALCOHOL
Alcohol has been used by people for a very long time. Archaeological evidence suggests that beer was brewed in Neolithic times and that drinking has always been a social practice (Social Issues Research Centre, 1998). The earliest known set of written laws, the code of Hammurabi, named for the Babylonian king responsible for them (circa 1790-1750 BCE), sets out a number of regulations around alcohol. Many different practices and expectations around alcohol have developed in different countries. For example, many southern European countries have what can be described as an everyday drinking culture, whereby alcohol is consumed regularly, in small amounts, usually with food. In contrast, most ‘celebratory’ patterns of drinking have been traditionally associated with northwestern Europe: alcohol is not consumed daily (and sometimes infrequently), but large amounts are consumed at special occasions or weekends (see Measham, 2006). It is important to consider alcohol within its social context.
There have been some changes in drinking patterns over the past 10 years or so. The Institute of Alcohol Studies estimated UK alcohol consumption to be 7.77 litres per person in 2013. This is less than the 2004 peak of 9.5 litres, and there has been a general downward trend since then. In Ireland too, per capita consumption has decreased in recent years and was 10.7 litres per person in 2013 (Alcohol Action Ireland 2015), but this remains higher than the OECD average of 9.2 litres. The UK Office for National statistics reports that in 2013, 21 per cent of adults reported that they do not drink alcohol, up from 19 per cent in 2005. Much of this change seems to be driven by younger people. The proportion of young adults in the UK who report drinking frequently is down by two-thirds since 2005. Binge drinking is also down, and again young adults are primarily responsible: in 2013, 18 per cent of young adults reported binging in the week before the interview, compared with 29 per cent in 2005.
Nevertheless, while many people use alcohol responsibly, its misuse and abuse is a social major problem. The cost to the National Health Service (NHS) in England and Wales is estimated to be £3.5 billion annually, and approximately 1.4 per cent of deaths are likely to be alcohol related (ONS, 2015). Irish data suggest that alcohol caused 4.4 per cent of deaths between 2000 and 2004, and a quarter of deaths in young men (Department of Health, 2012). Data from the 2012/13 and 2013/14 Crime Survey of England and Wales indicate that approximately 70 per cent of violent incidents at the weekend or during the evening are linked to alcohol and that the associated injuries are more likely to be severe. Further, alcohol has well-known negative effects on mental health. It has been estimated to contribute to approximately 50 per cent of suicides and is associated with self-harming behaviour (Department of Health, 2012).
Public health authorities recommend safe drinking levels. In terms of volume, it is recommended that women drink no more than 14 units per week and men no more than 21. In the UK a unit is defined as 8 g (10 ml) of pure alcohol. A unit equals a small glass (125 ml) of wine, UK pub measure of spirits or a half-pint of standard-strength beer. Box 10.3 (p. 235) explains how to calculate the number of units in an alcoholic drink.
However, for some time there has been a focus on safe drinking practices rather than total weekly consumption, as it is increasingly being recognised that binge drinking is harmful (see Box 10.1 - What is a binge?). The UK Department of Health recommends daily benchmarks, rather than weekly limits. These are 2-3 units for women and 3-4 units for men. People are advised not to drink heavily on a single occasion and a number of alcohol-free days each week are recommended.
Alcohol enters the circulation quickly and is absorbed in about 2 hours. It has wide-ranging effects on the central nervous system (CNS) and tends to depress CNS and behavioural activity. However, it is now clear that some parts of the brain are particularly vulnerable to the effects of alcohol (Lee et al., 2009). It affects the action of the neurotransmitters GABA and glutamate. In common with other addictive drugs, alcohol stimulates the release of the neurotransmitter dopamine from the nucleus accumbens (Boileau et al., 2003). This is an important source of positive reinforcement that acts to maintain drinking. At low and moderate doses, alcohol reduces anxiety (anxiolytic effect) and this may be a source of negative reinforcement (i.e. the removal of anxiety reinforces the drinking behaviour).
Table 10.3 Many factors determine the effect a given dose of alcohol will have on an individual. These factors include biological characteristics and predispositions, lifestyle, health, psychological and social context. Some of these factors are stable, such as gender, while others, such as mood, are liable to change
|
Factors that affect the response to alcohol include: |
|
✵ Genetics ✵ Gender ✵ Age ✵ Body size and composition ✵ Habitual alcohol consumption ✵ State of health ✵ Mood and expectancies |
EFFECTS OF ALCOHOL ON COGNITION
The negative impact of alcohol on cognition and psychomotor function is often painfully obvious in most town and city centres on Friday and Saturday nights. That alcohol impairs cognition is beyond question. Research is concerned with questions such as the nature and degree of the impairments, the level of alcohol required to cause them and the impact of drinking patterns on cognition.
Many authors have suggested that the effects of alcohol on performance become more detrimental as performance becomes more complex, though it is difficult to draw firm conclusions as the definition of complex can vary between studies. A number of studies have shown alcohol to impair memory; however, low doses of alcohol may improve performance by reducing anxiety (Streufert and Pogash, 1998). Lamberty et al. (1990) found that alcohol administered post-trial actually improved recall of prose passages, although this might be explained in terms of alcohol inhibiting the consolidation of memories after it is ingested. Streufert and Pogash (1998) have emphasised the need to examine the effects of alcohol on real-life complex tasks, outside the laboratory.
Box 10.1 What is a binge?
The term binge drinking is widely used. Any kind of binge implies a bout of excessive indulgence, be it in food, drink or anything else. But what counts as a drinking binge? What would you consider to be binge drinking?
Berridge et al. (2009) point out that the notion of a drinking binge has changed: it used to mean an extended period of heavy drinking but now refers a single session of risky drinking
There are different approaches to defining binge drinking. Volume-based definitions focus on the volume of alcohol consumed.
✵ US research typically defines a binge as the consumption of four (women) or five (men) standard drinks in a row.
✵ In the UK, volume-based definitions of eight or more units for men and six or more for women, in a single session, have been used. Subjective definitions, in contrast, are concerned with the effects, so a binge would be defined in terms of whether drinking led to drunkenness. So,
✵ Have you felt drunk in the past week?
Activity: Identify the advantages and disadvantages of (i) volume-based and (ii) subjective definitions of binge drinking. Which do you think is more useful? Why? Can you find any evidence to support this choice?
Box 10.2 Improbable alcohol research
The Ig Nobel prize is awarded for ‘… achievements that first make people laugh, and then make them think’. They were created by Marc Abrahams, founder of The Annals of Improbable Research. See www.improbable.com/ig/
Laurent Bègue and colleagues won the 2013 Psychology Ig Nobel for their study: ‘Beauty is in the eye of the beer holder: People who think they are drunk also think they are attractive’.
The phenomenon of ‘beer goggles’ is well known, whereby alcohol intoxication makes potential romantic partners look more attractive than they might appear when the observer is sober! However, Bègue et al. (2013) examined the effect of alcohol on people’s perceptions of their own attractiveness. They conducted the study in a French bar and measured alcohol level using a breathalyser. Unsurprisingly, they found that the more alcohol was consumed, the more attractive participants rated themselves! To try to disentangle the effects of alcohol from the effects of expectancies, the researchers conducted an experiment in which eighty-six men were recruited and assigned to one of four conditions:
✵ given alcohol, told drink was alcoholic;
✵ given alcohol, told drink was non-alcoholic;
✵ given non-alcoholic drink, told it was alcoholic;
✵ given non-alcoholic drink, told it was non-alcoholic.
They then filmed a short message advertising the drink. The men themselves then rated their performance in terms of attractiveness, originality and so on. Each film was also rated by an independent observer. Those who thought they had consumed alcohol (regardless of whether they had) rated themselves as more attractive; however, these ratings were not correlated with those of the independent judges. They researchers concluded: ‘In summary, the present research shows that alcohol-related expectancies can significantly boost self-perceived attractiveness. However, the perceived attractiveness lies in the eyes of the “beer holder” and is not shared by anyone else’ (p. 232).
In another study, Duke and Bègue (2015) looked at the relationship between blood alcohol concentration (BAC) and moral reasoning in the ‘trolley problem’. The trolley problem is a well-known ethical dilemma with two versions.
A runaway trolley is heading for five people and will kill them.
Version 1: you can stop it by flipping a switch that diverts it onto another track, but there is one person on this track.
Version 2: you can stop it by pushing a large man into the path of the trolley.
Essentially the problem asks whether it is acceptable to sacrifice one life to save five. A utilitarian approach to ethics judges the morality of action in terms of its consequences, so it would be acceptable. A deontological approach is more concerned with rules or duties, and it would not permit the sacrifice. Interestingly, studies seem to suggest that most people will choose the utilitarian option (i.e. flip the switch) for version 1 but not for version 2. You might like to try this with family and friends.
There has been a fair bit of psychological research examining the contribution of, on the one hand, deliberative reasoning, and on the other, empathy and emotional response, to these kinds of decision. Given that alcohol impairs reasoning, Duke and Bègue were interested in the effect on responses to the dilemma.
This study also took place in a French bar. The results showed that the more participants had drunk (the higher the BAC) the greater their willingness to choose the utilitarian option in version 2, i.e. to push the man into the path of the trolley. Given that alcohol impairs deliberative reasoning, these findings indicate that the utilitarian response is not explained by higher cognitive processes (as some have claimed). The authors suggest that alcohol decreases an aversion to harming others, and this explains the response.
Further reading
Bègue, L., Bushman, B.J., Zerhouni, O., Subra, B. and Ourabah, M. (2013). ‘Beauty is in the eye of the beer holder’: people who think they are drunk also think they are attractive. British Journal of Psychology, 104, 225-234.
Duke, A.A. and Bègue, L. (2015). The drunk utilitarian: blood alcohol concentration predicts utilitarian responses in moral dilemmas. Cognition, 134, 121-127.
METHODOLOGICAL ISSUES IN RESEARCH ON ALCOHOL AND COGNITION
Individuals vary greatly in their response to alcohol, and in their habitual alcohol consumption. There are differences between individuals in the effects of alcohol; for example, a given dose of alcohol tends to have more effect on a woman than on a man of the same weight, as men’s bodies contain more water and water tends to dilute the alcohol. Similarly, older adults tend to have less lean tissue than younger adults, so a given dose of alcohol is likely to have greater effects. Other factors include age, body size and composition, genetics and habitual alcohol consumption. A given individual may also have a different response to alcohol at different times, and this may depend on stomach contents, time of day, mood, hormonal levels and factors such as stress, expectancies, state of health and the situation.
As in the case of caffeine, the range of methodologies used by researchers further complicates the picture. Studies vary in terms of participants, alcohol doses, methods of administration and controls used. A vast range of dependent variables has been studied and these tasks differ in terms of length and complexity. A further complication is expectancy - people expect alcohol to impair their performance and may behave ‘drunk’ because they expect to be intoxicated. Placebos are routinely used to try to establish the effects of expectancy (see example in Box 10.2), but it is difficult to persuade people that they are drinking alcohol when they are not. Evidence suggests that placebo effects of alcohol are very variable and may reflect efforts to compensate for deficits in expected performance (see Testa et al., 2006).
Box 10.3 How to calculate the number of alcohol units in a drink
How many units?
The number of units in your drink depends on the size of the drink (volume) and the alcohol content of the beverage. The alcohol content is alcohol by volume or ABV, and this information should be on the bottle.
Volume (ml) * ABV /1000
So a large, 175 ml glass of wine with an ABV of 12.5 per cent has
175 *12.5/1000 = 2.19 units.
However, if the wine has an ABV of 14 per cent, there will be 2.45 units. Most wines have ABVs of 12-15 per cent, and pub or restaurant measures of 150, 175 or even 250 ml are common. This means that it is quite rare to find a glass of wine that has one unit of alcohol.
A UK pub measure (25 ml) of spirit is one unit of alcohol. An Irish pub measure is larger (35 ml). Of course, people tend to serve themselves much larger measures at home. Spirits such as vodka, gin and brandy typically have an ABV of around 40 per cent. A 60 ml measure of vodka would give you 2.4 units.
ALCOHOL AND PERFORMANCE
Teaction Time
The effects of alcohol on reaction time have been well researched, and it is clear that it does impair reaction time. This impairment is mediated through central, cognitive processes rather than peripheral motor processes (e.g., Kerr et al., 1991). Alcohol also impairs both visual pattern recognition and visual attention. Nonetheless, some studies have found no effect of alcohol on performance (e.g. Kerr and Hindmarch, 1991).
Alcohol and driving performance
The effects of alcohol on driving ability have been well investigated as alcohol is a major contributor to road traffic accidents, as well as other kinds of accident. Most jurisdictions prohibit driving while under the influence of alcohol. Blood alcohol concentration is used to detect this and enforce the prohibition. In England and Wales, the BAC limit is 0.08: that means that if more than 80 mg of alcohol per 100 ml blood is detected, the driver is ‘over the limit’ and can be charged with an offence. This limit is higher than in most other EU countries, which typically have limits of 50 mg/100 ml. The trend is towards lowering the limit; both Ireland (in 2010) and Scotland (in 2014) have reduced theirs from a BAC of 0.08 to a BAC of 0.05. It is worth noting that considerable progress has been made in raising awareness of the issue, and driving under the influence is no longer considered to be in any way acceptable by the vast majority of people. UK Department of Transport figures suggest that drink-related road deaths in 2013 were six times lower than in 1979. Nevertheless, alcohol remains a significant contributor to road fatalities and casualties.
Studies have tended to use driving simulators, or focus on tasks that assess components of driving such as coordination, complex reaction time, divided attention and so on. Research has clearly demonstrated that alcohol impairs the components of driving behaviour (e.g. Kerr and Hindmarch, 1998). It disrupts behaviours that are crucial in vehicle control, such as brake reaction time and steering. These impairments can be seen even at moderate and low doses of alcohol (Kerr and Hindmarch, 1998). Indeed, it is clear that alcohol concentrations greater than 0.05 cause significant psychomotor impairment (Brumback et al., 2007). Alcohol also increases the likelihood that a driver will take risks (Burian et al., 2002). It produces a narrowing of attention, so that individuals tend to focus on the most salient components of a task or stimulus (Harvey, 2015), such as steering, at the expense of other aspects, such as road awareness. People driving under the influence of alcohol often deny that their performance is harmed, because the narrowing of attention to one or two components of driving leads to a subjective feeling of competence. This is very much at odds with the objective reality: driving performance is always impaired after alcohol consumption. Worryingly, evidence indicates that heavier drinkers underestimate the extent of their alcohol-induced psychomotor impairment relative to lighter drinkers (Brumback et al., 2007). Even at a BAC of 0.05, which is lower than the current legal limit in England and Wales, driving ability is impaired (Kerr and Hindmarch, 1998).

Figure 10.4 A unit of alcohol is the amount in a standard (125 ml) glass of wine, a UK pub measure of spirits or half a pint (approx. 260 ml) of standard-strength beer or cider (3.5-4 per cent). Bear in mind that many beers and ciders are stronger than this, so half a pint of a strong lager contains more than 1 unit. Alcopops typically contain 1.5-1.7 units, depending on the brand, though some may be stronger.
Source: copyright Older Brother/Shutterstock.com.
Alcohol and memory
Acute doses of alcohol seem to exert most effects on working memory, whereas chronic exposure to alcohol impairs long-term memory (Molnár et al., 2010). Certainly a single episode of heavy drinking can have deleterious effects on memory, causing a ‘blackout’: ‘An alcoholic blackout is amnesia for the events of any part of a drinking episode without loss of consciousness’ (Lee et al. 2009, p. 2785).
Drinking fast on an empty stomach increases the risk of a blackout, but some people seem to be more vulnerable to them than others. A blackout involves the disruption of the encoding of episodic memory. Evidence suggests that the effects of alcohol on CA1 pyramdial cells of the hippocampus may be an important mechanism underlying this problem (Lee et al., 2009). While blackouts occur in non-alcoholics, Lee and colleagues suggest that the way that people respond to blackout, by changing their drinking behaviour or not, predisposes them to risk of greater alcohol abuse.
Given the association between alcohol, violence and crime, the effects on eye witness recall are of particular real-world importance. This was investigated by Hagsand et al. (2013). One hundred and twenty-six participants were allocated to a no, low or high alcohol condition and watched a mock crime scene. They were asked to recall what they had seen one week later. Those in the high alcohol condition recalled less detail but there was no difference in accuracy between the groups. However, for ethical reasons the doses of alcohol used were low and the ‘high’ dose was a BAC of 0.06 (again, below the driving limit in England and Wales at time of writing). The authors also caution about the degree to which the emotional response to a real crime scene might affect memory.
Habitual alcohol consumption and cognition
Excessive use of alcohol is associated with cognitive deficits and neurological damage, but it is not clear when moderate social drinking can become harmful. The picture is further complicated by the fact that definitions of social drinking, alcohol abuse and alcoholism are not stable and have changed over time, differ between countries and are used in different ways by researchers.
In 1971, Ryback put forward the continuity hypothesis, which held that there is a continuum of negative alcohol effects, from small, often undetectable, cognitive deficits in social drinkers to alcoholic dementia and Korsakoff’s syndrome. These effects are the result of alcohol-induced brain damage. Others have suggested that small amounts of alcohol do not cause damage and that it is the consumption of large volumes of alcohol in a single sitting (binge drinking) that is responsible for brain damage (see Nichols and Martin, 1998). Certainly evidence does show that binge drinking is associated with deficits in attention, memory and psychomotor performance (Lisdahl et al., 2013). However, when we take light or moderate social drinking the evidence is very mixed: some research has suggested associations between low levels of alcohol consumption and poor cognitive performance, whereas other work indicates no, or even beneficial, effects of light to moderate alcohol use (see Panza et al., 2012).
Leroi et al. (2002) conducted a 13-year follow-up of 1488 participants who had participated in the Epidemiologic Catchment Area study. Cognitive function was assessed at using the Mini Mental Status Examination (MMSE) at time 1 (1981), time 2 (1982) and time 3 (1993-96). Information about drinking behaviour was also collected. Mean MMSE scores showed decline across time, but this decline was greater for non-users for alcohol, particularly for women. Supporting this, on the basis of a substantial literature review, Panza et al. (2012) concluded that there was evidence to suggest a protective effect of low to moderate alcohol consumption on dementia. The potential mechanisms of this effect are multiple, but include a reduction in risk of brain infarcts and lesions to white matter. However, the picture is a very complex one. Alcohol use is confounded with many other lifestyle factors that influence the risk for dementia, and much of this work is cross-sectional in nature, with all the associated limitations. Whether or not alcohol has a protective effect may depend on individual genetic susceptibility to dementia and to the effects of alcohol (Panza et al., 2012). While much of this work focuses on older adults, other work suggests that use of alcohol early in life may have a greater neurocognitive impact on the developing nervous system (Lisdahl et al., 2013). Clearly, more research is needed.
The picture is clearer regarding heavy and abusive use of alcohol; this impairs a wide range of cognitive functions. Binge drinking in adolescents and young adults is associated with deficits in attention, memory and psychomotor speed (Lisdahl et al., 2013). The mechanisms underpinning these negative effects are likely to be the neurotoxic effects, negative effects on blood flow and metabolism in the central nervous system and nutritional deficiencies associated with alcoholism (Lisdahl et al., 2013). For example, Korsakoff’s syndrome is a form of amnesia caused by thiamine (vitamin B1) deficiency, which causes damage to the brain, particularly to the mamillary bodies. Korsakoff’s syndrome is characterised by both reterograde and anterograde amnesia (Victor, 1992). Patients have great difficulty acquiring new information, such as the name of their doctor, though short-term memory is usually preserved. There may be impairments in other cognitive functions, but these are minor in comparison with the memory deficit and it is worth noting that implicit memory and procedural memory are general preserved. The condition can be treated via administration of thiamine and resumption of a normal diet, and it is estimated that about a quarter will make a good recovery (Alzheimer’s Society, n.d.).

Figure 10.5 Alcohol always impairs driving. Research has identified three key ways in which this happens: impaired vehicle control, narrowed attention and greater risk taking.
Source: copyright Trueffelpix/Shutterstock.com.
CONCLUSIONS
Alcohol generally impairs a wide range of cognitive functions. Heavy drinking, binge drinking and alcoholism are reliably associated with cognitive deficits. The age at which someone starts drinking is likely to be important. As the brain is still developing in adolescence, alcohol is likely to have a greater neurocognitive impact. The picture regarding low to moderate alcohol consumption is mixed, and there is considerable variation in the ways that researchers define and measure moderate drinking. However, on balance, the evidence to date does not indicate that social drinking harms cognition, and it may even have some protective effects in later life for some people. Overall, we can conclude that:
✵ Alcohol tends to affect performance negatively, especially on complex tasks.
✵ Alcohol always impairs driving performance.
✵ It can lead to concentration on main skill components to the detriment of secondary ones.
✵ More research is needed on the impact of alcohol consumption throughout the lifespan.
10.4 NICOTINE
Nicotine is an alkaloid and is the key active ingredient in tobacco, which is most commonly smoked in the form of cigarettes, but can also be smoked in cigars and pipes or chewed (chewing tobacco and paan). More recently, e-cigarrettes have become popular, particularly as an aid to smoking cessation. These battery-operated ‘cigarettes’ allow users to inhale nicotine as a vapour. The 1988 US Surgeon General’s Report (USDHHS, 1988) classified nicotine as an addictive substance and drug of abuse for the first time. It is now generally accepted that nicotine is addictive and largely responsible for the tenacity of the smoking habit.
Smoking rates have declined steadily since the 1970s and smoking is now a minority activity. In the UK, adult smoking rates have dropped from approximately 24 per cent in 2007 to 18 per cent in 2015. Yet smoking remains the biggest single cause of preventable death in the UK and Ireland. It has been estimated to be responsible for approximately 18 per cent of deaths of adults over 35 years (Health and Social Care Information Centre, 2010).
Nicotine acts as an agonist for the neurotransmitter acetylcholine (ACh). There are two kinds of receptor for acetylcholine, the muscarinic and the nicotinic. Nicotine acts as an agonist at the nicotinic receptor, hence the name. Cholinergic systems (systems of neurons that use ACh as a neurotransmitter) are important in cognition, and cholinergic agonists (e.g. hyoscine, nicotine) tend to improve cognitive performance while cholinergic antagonists (e.g. scopolamine, mecamylamine) tend to impair it (Levin, 1992). Alzheimer’s disease is associated with a loss of nicotinic cholinergic receptors in the CNS, and this is linked to the development of the characteristic plaques (Newhouse et al., 2004). This and other observations led to the cholinergic hypothesis of cognitive decline: age-related cognitive decline is the result of decline in CNS cholinergic activity, often due to death of cholinergic neurons, particularly in the basal forebrain. The failure of cholinergic agents to halt or reverse AD progress or to improve non-pathological age-related cognitive decline undermined this approach, but neuroimaging studies have helped to clarify that cholinergic processes do play a role, particularly in directing and modulating attention (Dumas and Newhouse, 2012). It is important to note that smoking is a significant risk factor for the development of AD (see Cataldo et al., 2010).
NICOTINE AND COGNITION
Experimental work on nicotine and cognition has two main foci. The first is to use nicotine as a tool to examine the role of nicotinic cholinergic systems in cognition. The second major focus is to try to understand why people smoke and to develop pharmacological and behavioural aids to smoking cessation. Given the evidence discussed in the previous section, we might expect nicotine to improve cognitive performance, but much of the evidence has been contradictory. Of course, studies of the effects of nicotine on humans are complicated by the fact that some people smoke and others don’t. In a review of the literature on human studies, Newhouse et al. (2004) concluded that much of the research on the effects of nicotine on non-smokers tends to show no effects or negative effects, whereas studies that examine the effect of nicotine in populations with pathologies such as AD, Parkinson’s disease and so on tend to find that nicotine enhances cognitive performance. They concluded:
If an individual subject is performing suboptimally because of a disease state or impairment (e.g. AD), his performance will be enhanced by increased nicotinic stimulation … However, if an individual subject is already performing at or near their optimal level of performance, increasing nicotinic stimulation will produce deterioration in cognitive functioning.
(p. 42)
Many studies have compared the effects of nicotine (delivered through smoking) in abstinent and non-abstinent smokers. However, it is difficult to compare the effects of nicotine in smokers and non-smokers: the effects of an acute dose of nicotine will be different in smokers and non-smokers, because smokers have had chronic exposure to nicotine and smokers are a self-selected population and may differ in other relevant ways (including response to nicotine). Nonetheless, it is clear that smoking reliably improves the performance of abstinent smokers. Three hypotheses have been proposed to account for this. The Nicotine Resource Model holds that the gains in performance are due to the beneficial effects of nicotine per se, i.e. nicotine acts to improve performance. The Deprivation Reversal Model purports that gains in performance represent the alleviation of withdrawal symptoms that impair performance, rather than true gains. The Combination Hypothesis proposes some combination of the two. In an effort to try to differentiate enhancement and alleviation of withdrawal, Heishman et al. (2010) conducted a meta-analysis of studies that investigated the effect of either nicotine or smoking on adults who were not, or were only minimally, nicotine deprived. They found evidence of genuine enhancement on some aspects of motor performance, attention and memory.

Figure 10.6 Smokers self-administer nicotine on a regular basis and smoking is a particularly effective method of drug administration, allowing fingertip control of dosage. The amount of nicotine a smoker receives depends on the number of puffs taken and the depth of inhalation. Therefore it is difficult to infer the extent of tobacco dependence on the basis of number of cigarettes or strength of cigarettes smoked. When smoked in the form of tobacco, nicotine enters the circulation quickly and reaches the central nervous system in approximately 10 seconds (Le Houezec, 1998).
Source: FreeImages.com/mi-sio.
REACTION TIME
Smoking has been shown to both improve reaction time and decrease errors in smokers (see Pritchard and Robinson, 1998). Nonetheless, some studies have found smoking to impair reaction time (e.g. Frankenhauser et al., 1970). The rapid visual information processing (RVIP) task is a form of choice reaction time task that has been studied extensively in relation to smoking and nicotine. It consists of the fast presentation of a series of digits on a computer screen. Participants are required to press a response key when they detect three consecutive odd or even numbers. Performance can be assessed using three measures: the number of correct responses; the average time taken to respond to a target (reaction time (RT)); and the number of errors made. Wesnes and Warburton (1983) found that smoking improved both speed and accuracy. A subsequent study obtained the same effects using nicotine tablets (Wesnes and Warburton, 1984). Warburton and Mancuso (1998) also reported positive effects of a transdermal nicotine patch. However, Wesnes and Revell (1984) failed to find an effect of nicotine (1.5 mg tablets) on RVIP in non-smokers, though they attributed this to methodological issues.
LEARNING AND MEMORY
Evidence regarding the effects of nicotine on short-term memory (STM) is inconsistent. A number of studies have reported that nicotine increases speed of short-term memory scanning (e.g. Sherwood et al., 1992), but not accuracy. However, in a meta-analysis, Heishman et al. (2010) found evidence that nicotine enhances short-term but not long-term episodic memory accuracy. There was no evidence of any effect on working memory accuracy, but working memory reaction time was enhanced.
Much animal work has suggested that nicotine facilitates learning on a wide range of tasks. Nicotine delivered through smoking or other routes has been reported to improve performance on a number of learning tasks, including free recall, paired-associate learning, serial recall, retention of nonsense syllables and recall of prose (see Pritchard and Robinson, 1998). Despite this, a number of studies have found no effects or negative effects of nicotine on learning and memory.
Little work has focused on cognitive strategy or style, rather than overall performance. Algan et al. (1997) found that smoking affected problem-solving strategies in women, but not in men. In contrast, smoking improved the speed and accuracy of performance on a verbal task for men only. Further research is clearly needed in this area.
ATTENTION
Many studies have demonstrated nicotine-related enhancements of cognition and, again, smoking reliably improves attention in smokers. Smoking and nicotine gum have been shown to improve both visual and auditory signal detection. The effects of nicotine/smoking on the Stroop effect have been well investigated, and nicotine gum has been reported to reduce the interference, that is, the size, of the Stroop effect (Provost and Woodward, 1991). However, some researchers have failed to find any effects of nicotine on the Stroop effect (e.g. Parrott and Craig, 1992), though Pritchard and Robinson (1998) suggest that this may have been due to an insufficient number of trials. Some researchers have suggested that attention mediates the effects of nicotine on learning and memory, so that any improvement may be at least partly the result of improved attention. Heishman et al. (2010) found positive medium effects of nicotine on alerting attention accuracy, reaction time and orientating attention reaction time, but not accuracy. These seem to reflect enhancements rather than alleviation from withdrawal.
IMPLICATIONS
It is clear that nicotine withdrawal is associated with declines in cognitive performance in smokers. This may be a factor in making abstinence difficult and an inducement to continued smoking. Arousal modulation models of smoking maintain that smokers smoke in order to maintain preferred or optimal levels of arousal, performance and mood, and much of the evidence seems to fit well with this. However, questions still remain. It is generally assumed that any performance gains after smoking are due to the action of nicotine, yet there is no hard evidence to support this and few studies have actually measured actual intake or blood levels (Le Houezec, 1998). Tobacco contains many active ingredients, and few have been studied in relation to humans. Moreover, smoking is a complex behaviour, and non-pharmacological aspects of smoking could be responsible or at least partly responsible for the observed improvements in performance. For example, there is evidence that smokers’ expectancies may affect their response to smoking (Juliano et al., 2011). It is important to understand the role of these effects in maintaining the smoking habit, yet most laboratory studies have used acute doses of nicotine despite the fact that smoking is characterised by chronic nicotine use. The effects of long-term chronic nicotine exposure on cognition have not been well investigated. Moreover, it must be remembered that smoking is a complex behaviour: there is more to it than nicotine. Physiological, cognitive, personality and wider social variables have all been implicated in recruitment, maintenance, cessation and relapse. We need a deeper understanding of the non-pharmacological effects of smoking on cognitive performance.
CONCLUSIONS
The effects of nicotine on cognitive performance are generally positive; particularly in populations with pathologies. However, smoking is a significant risk factor for dementia. While smoking certainly improves the cognitive performance of abstinent smokers in the short term, there is evidence to suggest that there are genuine effects of nicotine on attention and memory that cannot be attributed to alleviation from withdrawal (Heishman et al., 2010; Pritchard and Robinson, 1998). Overall we can conclude:
✵ There are positive effects of nicotine on attention and some aspects of memory.
✵ Smoking reliably improves the cognitive performance of abstinent smokers.
✵ The effects of nicotine/smoking on cognition probably play a part in maintaining the smoking habit, but other factors are also important.
✵ Smoking is a significant risk factor for the development for AD.
10.5 INTERACTIVE EFFECTS OF THE SOCIAL DRUGS ON COGNITION
In everyday life, the social drugs are used in combination. Smokers tend to smoke more while drinking coffee and alcohol (Istvan and Matarazzo, 1984). Alcohol and caffeine are consumed together in the form of mixed drinks (e.g. vodka and cola) or liqueur coffee, and of course people use coffee to ‘cure’ a hangover. Surprisingly, this is a very under-researched area - little is known about the interactive effects of the social drugs.
ALCOHOL AND NICOTINE
Alcohol is reliably associated with increased cigarette consumption (Istvan and Matarazzo, 1984) and indeed most smokers report smoking more than usual when drinking alcohol. There is some evidence that nicotine may help to counteract performance deficits resulting from low doses of alcohol, particularly on simple tasks (Kerr and Hindmarch, 1998). However, the picture is not clear-cut by any means. Studies have reported antagonistic, synergistic, null and mixed effects of this combination on cognitive performance (see Kerr and Hindmarch, 1998).
ALCOHOL AND CAFFEINE
Caffeine is often used as a cure, and can counteract effects of very low doses of alcohol (e.g. Pihl et al., 1998). Even at low doses, alcohol impairs dual-task performance. The addition of caffeine has been shown to reduce alcohol-related interference in these tasks but not the alcohol-induced reductions in accuracy (Marczinski and Fillmore, 2006). There is no clear evidence of caffeine as a ‘cure’ for overindulgence in alcohol. Howland et al. (2011) examined the interactions between caffeine and alcohol on driving behaviour in a simulator, with 127 students each allocated to one of four conditions:
✵ alcoholic beer;
✵ alcoholic beer + caffeine;
✵ non-alcoholic beer;
✵ non-alcoholic beer + caffeine.
Alcohol significantly impaired driving performance, but the addition of caffeine made no difference to this. Certainly the evidence does not suggest that caffeine can be used to counteract the negative effects of drinking on performance.
NICOTINE AND CAFFEINE
Very few studies have examined the interactions between nicotine and caffeine, despite the fact that they are frequently used together in everyday life. Evidence suggests that the interactions between nicotine and caffeine are complex (Johnson et al., 2010). Smokers are more likely to be coffee-drinkers than non-smokers and they tend to consume more coffee. The relationship is unlikely to have a pharmacological basis as studies have demonstrated that, in smokers, caffeine intake does not affect the level of smoking (e.g. Lane and Rose, 1995). Both nicotine and caffeine have been shown to improve performance, but these effects do not seem to be additive: nicotine and caffeine together do not produce a greater effect than either substance alone (Kerr et al., 1991).
CONCLUSIONS
There is a real shortage of research in this area. It is difficult to draw firm conclusions on the basis of existing research, as studies cannot easily be compared owing to differences in methodologies.
10.6 THE EFFECTS OF THE SOCIAL DRUGS ON COGNITION: A SUMMARY
The social drugs do affect cognitive performance in fairly predictable ways, but methodological variations have made it difficult to compare studies directly and understand conflicting findings. The effects of these drugs on cognition are important, and it is crucial to understand their role in promoting and maintaining caffeine, alcohol and nicotine use. This research has also furthered our understanding of the neurobiology of cognition. It should be clear that use of these substances can act as a confounding variable in studies of cognitive performance, and it is important to control for them. Increased standardisation in empirical research will improve our understanding of the cognitive effects of the social drugs and the mechanisms underlying these effects. Overall, we can conclude:
✵ Caffeine tends to increase alertness and speed, particularly under sub-optimal conditions.
✵ Nicotine tends to improve attention and rapid visual information processing in smokers.
✵ In the cases of caffeine and nicotine, it is difficult to separate genuine enhancements and alleviation from withdrawal.
✵ Alcohol impairs a wide range of cognitive performance.
✵ Alcohol abuse is associated with neurological damage.
✵ Interactions between the three are complex and have not been not well investigated.
✵ There are problems comparing studies as methodologies are not equivalent.
10.7 CANNABIS
Cannabis, also known as marijuana, is usually derived from either the cannabis sativa or cannabis indica plants (Figure 10.7). It is usually taken in the form of dried leaves and flower heads, or the resin secreted by these. It can be eaten, but is more usually smoked in the form of a cannabis cigarette, or joint, often mixed with tobacco, or in a pipe. It is the most commonly used illegal drug in England and Wales (see Table 10.4).
The active ingredients are carbon alkaloids known as cannabinoids. The most important of these is Delta9-tetrahydrocannabinol (D9-THC), and this is responsible for most of the effects of cannabis. These effects include enhanced perception, happiness, drowsiness, concentration and memory problems. As in the case of nicotine, smoking is a very effective method of drug delivery: a high proportion is absorbed and the effects are felt within seconds. The human body has natural (endogenous) receptors for the cannabinoids. The CB1 receptors are found in the CNS, particularly in the hippocampus, cerebellum and striatum (Ameri, 1999). The CB2 receptors are found on the cells of the immune system. Cannabis also triggers release of dopamine from the nucleus accumbens and this probably accounts for the reinforcing nature of cannabis use.
Cannabis has long been used for its medicinal properties. It has been shown to be effective in the management of chronic pain, particularly in conditions such as multiple sclerosis; however, it is a palliative rather than a cure (Bifulco and Pisanti, 2015). Twenty-three US states have legalised the medical use of cannabis (Bifulco and Pisanti, 2015) and a number (Crean et al., 2011) have decriminalised non-medical use. This is also the case in some EU states, for example The Netherlands, but cannabis remains illegal in the UK and Ireland. It was classified as a class B drug in the UK until 2004, when it was reclassified as class C. In 2008, this was reversed and it remains a class B drug under the Misuse of Drugs Act 1971.

Figure 10.7 The cannabis sativa plant. A shorter, denser plant, cannabis indica is also widely cultivated.
Source: FreeImages.com/Vitezslav Valka.
Table 10.4 The rates of past-year use of cannabis, cocaine and ecstasy based on responses to the 2013/14 Crime Survey in England and Wales
|
Cannabis use in the past year |
Cocaine use in the past year |
Ecstasy use in the past year |
|
6.6% of 16-59-year-olds |
2.4% of 16-59-year-olds |
1.6% of 16-59-year-olds |
|
15.1% of 16-24-year-olds |
4.2% of 16-24-year-olds |
3.4% of 16-24-year-olds |
|
7.9% of 25-34-year-olds |
4.2% of 25-34-year-olds |
2.3% 24-35-year-olds |
Source: Burton et al. (2014).
There are two main research designs employed in this research: examining the effects of acute doses of cannabis (smoked or eaten) on performance, or comparing the performance of cannabis users and non-users. Cannabis does impair attention, and heavy users are reported to have problems focusing attention and ignoring irrelevant information, and are easily distracted relative to controls (e.g. Solowij, 1995). Generally the evidence indicates that acute cannabis use impairs motor and cognitive function, but it is not clear how long these effects last (Crean et al., 2011).
MEMORY AND EXECUTIVE FUNCTION
Cannabis has been repeatedly shown to impair memory, particularly short-term memory. Millsaps et al. (1994) examined memory in cannabis-abusing teenagers and found it to be significantly impaired relative to general intellectual level. These negative effects are assumed to result largely from the effects of cannabis at the CB1 receptors in the brain, particularly in the hippocampus. There is also evidence that the cannabinoids can act as neurotoxins and cause cell death (Ameri, 1999). Rodgers et al. (2001) developed a website to evaluate the effects of drug use on self-reports of memory ability. Memory was assessed using the Prospective Memory Questionnaire and the Everyday Memory Questionnaire. Cannabis use predicted everyday short-term cognitive problems, while ecstasy use predicted long-term memory difficulties that seem to be the result of problems in retrieval and storage.
It is not clear how persistent the effects are. A number of authors have suggested that cannabis-related deficits persist even after long periods of abstinence (e.g. Solowij, 1995), but others offer conflicting evidence. Pope et al. (2001) examined the performance of 108 long-term heavy cannabis users throughout a month of abstinence. Users showed memory impairments for at least 7 days, but by 28 days of abstinence they were not significantly different from controls. The authors concluded that the cannabis-related deficits are reversible with abstinence. However, more recent nueorimaging studies have indicated subtle, persistent impairments (see Crean et al., 2011). It can be difficult to examine the effects of cannabis clearly; it remains in the body for some time after ingestion, so it can be difficult to differentiate between acute effects and residual effects in the short term (days and weeks). Furthermore, heavy cannabis users often differ from controls in terms of lifestyle and other attributes that may well affect cognitive performance. Reviewing the research in the area on cannabis and executive function, Crean et al. (2011) reported that acute cannabis intoxication impairs working memory, attention, concentration and aspects of decision making. The degree of impairment seems to be greater for inexperienced users who have not developed tolerance. There is clear evidence that chronic heavy use of cannabis has long-term effects, even after abstinence, particularly on decision making and planning. Impairments in working memory and attention seem to be restored after abstinence. However, the age at which cannabis use begins may be important as regards long-term damage. Ehrenreich et al. (1999) examined the performance of ninety-nine cannabis users (they were not using other drugs and had no history of abusing other drugs) on various measures of attention. Cannabis use early in life was the most important predictor of impaired performance. These findings, and others, suggest that exposure to cannabinoids during early puberty can interfere with brain development and cause long-lasting neurological alterations.
CONCLUSIONS
Clearly cannabis use has deleterious effects on memory and attention and cannabis users show clear cognitive impairments relative to controls. There is concern that cannabis use may cause neurological damage resulting in persistent cognitive deficits, but the evidence is currently inconclusive. Certainly evidence does suggest that early use of cannabis may cause long-term cognitive problems. Overall we can conclude:
✵ Cannabis impairs memory, particularly short-term memory, and attention.
✵ It is not clear whether these impairments are long-term.
10.8 COCAINE
Cocaine is a CNS stimulant that is extracted chemically from the coca plant. The coca plant is native to South America and the leaves have been chewed for at least a thousand years (Snyder, 1996, p. 122). Pure cocaine was first isolated in Germany in 1860 and thereafter was widely used throughout Europe and America, often in drinks and tonics. Sigmund Freud was one of the first researchers to investigate its effects, and he recommended it as a cure for morphine addiction. Unfortunately, this treatment often resulted in cocaine psychosis, and there was a backlash from the medical establishment (Snyder, 1996, p. 128).
Cocaine is the second most widely used illegal drug in Europe (Vonmoos et al., 2013). In powder form it is inhaled or ‘snorted’, but cocaine can also be processed into a crystal form, ‘crack cocaine’, that is heated and smoked. Crack cocaine produces a more intense but shorter ‘high’ than powder cocaine. Use of either form is associated with significant physical and psychosocial risks (Sofuoglu and Sewell, 2009).
Cocaine is a stimulant, increasing energy and alertness. The subjective effects are euphoria, feelings of power, increased well-being and self-belief, increased energy and endurance, and little need for sleep or food. Both cocaine and amphetamines can cause ‘stimulant psychosis’. This psychotic state is similar to schizophrenia and sufferers often experience auditory hallucinations and feelings of paranoia. Cocaine increases the availability of the neurotransmitters dopamine, noradrenaline and serotonin, mainly by blocking monoamine transporters (Sofuoglu and Sewell, 2009). This action increases both central nervous system (CNS) and autonomic nervous system (ANS) arousal.
COCAINE AND COGNITION
Acute effects of cocaine have been examined in drug abusers, and occasionally in participants with no history of drug use. While acute doses of cocaine are associated with powerful subjective effects, the effects on performance are inconsistent. However, chronic or dependent cocaine use is reliably associated with cognitive deficits in attention, memory and executive function. In a systematic review of the acute and long-term effects of cocaine on cognition, Spronk et al. (2013) concluded that chronic cocaine use is assocated with impairments in attention, working memory, recall, cognitive flexibility and psychomotor function (see Table 10.5).
Research also suggests that recreational use is associated with impairments. Vonmoos et al. (2013) assessed attention, working memory, declarative memory and executive function in dependent cocaine users, recreational users and non-cocaine-using controls. Both groups of cocaine users showed impairments relative to controls, but impairment was greater for the dependent users. Evidence suggested that performance on memory and executive function was negatively correlated with duration and level of exposure to cocaine. Odds ratios were calculated and indicated that cocaine users had 3.8 times the risk of deficits than controls.
Prenatal exposure to cocaine (PEC) has been associated with cognitive deficits in later life. Animal work suggests that prenatal exposure can cause long-term memory damage (e.g. Morrow et al., 2002) and exposure in early infancy can impair spatial learning (Melnick et al., 2001). In a review of the effects of PEC on school-age children, Ackerman et al. (2010) found that the environment played a significant role in moderating the effects on language, cognition and academic performance. However, after controlling for these, impairments remained in sustained attention and behavioural self-regulation. An earlier meta-analysis found reliable effects only for motor performance and abnormal reflexes (Held et al., 1999).
Table 10.5 Key findings from Spronk et al.’s (2013) systematic review of the acute and chronic effects of cocaine on cognitive function
|
✵ Attention: mixed evidence regarding the acute effects but chronic use is associated with impairments to sustained attention. |
|
✵ Memory: little evidence that acute use impairs memory but chronic use is associated with recall deficits. The picture is mixed as regards working memory but visuospatial memory may be more affected than verbal, although more research is needed. |
|
✵ Cognitive flexibility: evidence of negative effects of chronic use. |
|
✵ Psychomotor performance: large impairments associated with chronic use. |
CONCLUSIONS
Chronic cocaine use is associated with cognitive deficits, particularly in executive function and decision making, but also in memory and language. It is unclear whether these effects reflect long-term neurological damage.
✵ Chronic use of cocaine and amphetamines is associated with deficits in decision making and executive function that resemble those of frontal and prefrontal cortical damage.
✵ Prenatal exposure to cocaine may cause deficits in attention and behaviour, but other effects seem to be mediated by the environment.
10.9 ECSTASY
Ecstasy is the everyday name for the synthetic amphetamine derivative MDMA (3,4-methylenedioxymethamphetamine). It achieved popularity at the end of the 1980s and was strongly associated with the ‘rave’ subculture (Figure 10.8). Ecstasy tablets often contain substances other than, or in addition to, MDMA, including amphetamines and amphetamine derivatives, caffeine, ketamine, codeine and ephedrine (Parrott, 2001). The subjective effects of ecstasy are powerful and are characterised by positive emotions and euphoria. MDMA acts as an agonist for the monoamine group of neurotransmitters (serotonin, dopamine, noradrenaline). These are important in mood and emotion; some anti-depressants work by inhibiting their reuptake. MDMA massively increases the availability of serotonin (Parrott, 2013) and blocks monoamine reuptake; this seems to be the neurochemical basis for the euphoria experienced by users. There are also physiological effects: increase in heart and respiration rates, and disruption of thermoregulation (the body’s ability to regulate its temperature). Hyperthermia has been the cause of a number of ecstasy-related deaths, usually exacerbated by hot and crowded dance venues. Many ecstasy users report mood disturbance, particularly feeling low or depressed, in the days following ecstasy use (Curran, 2000). This has been linked to ecstasy-induced depletion of serotonin, and there is concern about the potential long-term depressive effects. George et al. (2013) found that ecstasy use did not predict depression in a large-scale 4-year longitudinal study, but cautioned that the rates of ecstasy use in the sample were low. Animal studies have clearly demonstrated that ecstasy is a serotoninergic neurotoxin. The extent to which these findings are applicable to humans has been debated, as typically the doses used have been very high (Cole et al., 2002). Nonetheless, evidence from human neuroimaging studies increasingly indicates serotoninergic neurotoxic effects in humans (Parrott, 2013).

Figure 10.8 Ecstasy was associated with the rave/dance culture of the late 1980s and early 1990s.
Source: FreeImages.com/olddocks.
ECSTASY AND COGNITION
There is a good deal of research on the effects of ecstasy on cognitive function. Most studies have been concerned with the effects of chronic use and have compared the cognitive performance of ecstasy users and non-users: these studies are fundamentally correlational in nature. It must be remembered that ecstasy users are a self-selected sample and probably differ from non-users in other ways. People who use ecstasy often use other drugs as well, particularly cannabis, but some use a wide range of others, including cocaine, amphetamine and ketamine. This makes it difficult not only to choose a suitable control group but also to separate the effects of ecstasy from those of other recreational drugs used. Studies typically control for this statistically and/or via polydrug control groups (Parrott, 2013). Level of ecstasy consumption is usually based on participants’ self-reports and this can be problematic, particularly given the variations in MDMA levels in ecstasy tablets. A further problem is lifestyle differences between experimental groups: ecstasy users often have very disrupted sleep patterns and may spend long periods constantly awake, so discrepancies in performance between users and control groups may be due to these differences, rather than variations in drug usage. Different studies address these issues in different ways, and this may be, at least in part, responsible for some of the inconsistent findings (Bedi and Redman, 2008).
In general, studies have found no differences between ecstasy users and non-users on simple measures of performance, such as reaction time (e.g. Parrott and Lasky, 1998; see Parrott, 2013). Vigilance, visual scanning and attention also show few differences (e.g. Rodgers et al., 2001). However, deficits associated with ecstasy have been reported in memory and central executive function.
MEMORY AND EXECUTIVE FUNCTION
Many studies have reported memory impairments in chronic ecstasy users. Deficits have been reported in verbal recall (e.g. Morgan, 1999), working memory (Wareing et al., 2000) and prospective memory and central executive function (Heffernan et al., 2001). Morgan et al. (2002) reported impaired working memory and verbal recall in both current and ex-users of ecstasy, suggesting long-term damage. These deficits were predicted by amount of ecstasy use. Given that cannabis use is strongly associated with memory problems and that ecstasy users are often also cannabis users, a number of studies have attempted to disentangle the effects of the two on memory. It has been suggested that the frequently reported negative effects of ecstasy on memory are actually due to cannabis (Croft et al. 2001; Bedi and Redman, 2008). However, Gouzoulis-Mayfrank et al. (2000) found that ecstasy and cannabis users did worse than cannabis-only users and non-drug users, and Rodgers et al. (2001) found ecstasy and cannabis use to predict different kinds of memory deficit, as mentioned earlier.
In general, most of the empirical evidence suggests that ecstasy impairs cognition, and some findings suggest that it causes serious and long-lasting harm. In his 2013 review, Parrott reported deficits in retrospective memory, prospective memory and aspects of problem solving in abstinent ecstasy users. Generally, basic attention and working memory were not impaired. Degree of impairment seems to be related to exposure, with heavy users showing greater deficits. However, findings have been inconsistent (Bedi and Redman, 2008), often reflecting methodological differences, and in 2002 Cole et al. expressed concern that the media and some researchers report a causal relationship between ecstasy and cognitive impairment that has not in fact been established. Bedi and Redman (2008) reported small associations between ecstasy use and lower performance on some cognitive measures. In particular, they reported a negative correlation between lifetime ecstasy use and verbal memory performance. However, there was no evidence of a ‘clinical dysfunction’.
CONCLUSIONS
Overall the evidence suggests that ecstasy has deleterious effects on memory and executive function. Ecstasy is a neurotoxin that can cause irreversible neurological damage and long-term cognitive problems. Ecstasy users tend to perform significantly worse than non-users on tests of memory, particular verbal memory, and on a range of other executive functions. Basic lower-level cognitive skills are less affected than higherlevel ones, and impairments seem to be related to exposure. There is a need for more research to clearly establish cause-and-effect relationships and disentangle the effects of lifestyle and other drug use. Specifically we can conclude:
✵ ecstasy is a serotominergic neurotoxin;
✵ ecstasy users show reliable impairments in memory and central executive function;
✵ there is little evidence of impairment in lower-level cognitive function;
✵ the degree and duration of use seems to predict the level of impairment; and
✵ a clear cause-and-effect relationship has yet to be demonstrated in humans.
10.10 THE ILLEGAL DRUGS AND COGNITION: A SUMMARY
Cannabis, ecstasy and cocaine have negative effects on cognition, and these seem to be dose dependent to some extent. Animal work, particularly in the case of ecstasy, suggests that these substances may cause neurological damage that is reflected in cognitive deficits. Certainly chronic drug users and abusers show cognitive impairments relative to controls. The high frequency of polydrug use also makes it difficult to clearly identify the effects of a single drug, such as ecstasy. Of course, a good deal of this research is correlational in nature, although neuroimaging work is helpful in clarifying the neurological effects of drug use in humans. Well-designed, longitudinal research is needed to assess the long-terms effects of both chronic and recreational drug use on cognition.
SUMMARY
✵ Cannabis use is strongly associated with short-term memory and attention problems.
✵ Ecstasy use is associated with deficits in memory and executive function.
✵ Chronic cocaine use is also linked to impaired executive function and to poor decision making.
✵ These effects may be persistent and long-term; research needs to clarify this.
FURTHER READING
✵ Kanarek, R.B. and Lieberman, H.R. (2011). Diet, brain, behaviour: Practical implications. Florida: CRC Press.
✵ Preedy, V. R. (ed). (2012). Caffeine: Chemistry, analysis, function and effects. Cambridge: The Royal Society of Chemistry.
✵ Snel, J. and Lorist, M. (eds). (1998). Nicotine, caffeine and social drinking: Behaviour and brain function. Amsterdam: Harwood Academic.
✵ Wilson, S.J. (ed). (2015). The Wiley handbook on the cognitive neuroscience of addiction. Oxford: Wiley Blackwell.